 Tainá Carla Freitas de Macêdo1*
Tainá Carla Freitas de Macêdo1* Glescikelly Herminia Ferreira2
Glescikelly Herminia Ferreira2 Katie Moraes de Almondes3
Katie Moraes de Almondes3 Roumen Kirov4†
Roumen Kirov4† Sérgio Arthuro Mota-Rolim5*†
Sérgio Arthuro Mota-Rolim5*†- 1Department of Psychology, Federal University of Rio Grande do Norte, Natal, Brazil
- 2Department of Philosophy, Federal University of Pernambuco, Recife, Brazil
- 3Department of Psychology, Postgraduate Program in Psychobiology, Onofre Lopes University Hospital, Federal University of Rio Grande do Norte, Natal, Brazil
- 4Institute of Neurobiology, Bulgarian Academy of Sciences, Sofia, Bulgaria
- 5Brain Institute, Physiology and Behavior Department, Onofre Lopes University Hospital, Federal University of Rio Grande do Norte, Natal, Brazil
Nightmares are defined as repeated occurrences of extremely dysphoric and well-remembered dreams that usually involve subjective threats to survival, security, or physical integrity. Generally, they occur during rapid eye movement sleep (REMS) and lead to awakenings with distress and insufficient overnight sleep. Nightmares may occur spontaneously (idiopathic) or as recurrent nightmares. Recurrent nightmares cause significant distress and impairment in occupational and social functioning, as have been commonly observed in post-traumatic stress disorder, depression and anxiety. By contrast, during lucid dreaming (LD), subjects get insight they are dreaming and may even control the content of their dreams. These features may open a way to help those who suffer from nightmare disorder through re-significations of the dream scene, i.e., knowing that they are dreaming and having control over their dream content. Thus, lucid dreamers might be able to render nightmares normal dreams, thereby assuring a restoring sleep. The aim of the present study is to review the existing literature of the use of LD as an auxiliary tool for treatment of nightmares. We conducted a careful literature search for eligible studies on the use of LD treatment for nightmares. We observed that whereas LD may be a feasible aid in the treatment of patients with nightmares through minimizing their frequency, intensity and psychological distress, the available literature is still scarce and does not provide consistent results. We conclude therefore that more research is clearly warranted for a better estimation of the effective conductance and therapeutic outcome of LD treatment in clinical practice.
Introduction
According to the International Classification of Sleep Disorders, 3rd Edition (American Academy of Sleep Medicine, 2014), nightmare disorder represents repeated occurrences of extended, extremely dysphoric, and well-remembered dreams that usually involve threats to survival, security, or physical integrity. Nightmares generally occur during rapid eye movement sleep (REMS) and often result in awakening and worsened sleep quality. On awakening from nightmares, subjects rapidly become oriented and alert, but with emotional and physical signs of stress, such as fear, tachycardia, tachypnea, sweating, and daytime impairment in emotion regulation, cognition, and in many social areas of functioning (Levin and Nielsen, 2007; American Academy of Sleep Medicine, 2014; Scarpelli et al., 2019). Nightmares may occur occasionally in almost half of adults, but they may become recurrent, that is, repeated, especially in post-traumatic stress disorder (PTSD) (Hartmann, 1984; Aurora et al., 2010; Morgenthaler et al., 2018), anxiety (Haynes and Mooney, 1975; Levin, 1998; Nielsen et al., 2000; Zadra and Donderi, 2000; Tanskanen et al., 2001) and depression (Germain and Nielsen, 2003; Agargun et al., 2007).
An important etiological distinction made is the difference between idiopathic and posttraumatic nightmares. Idiopathic nightmares are those with unknown etiology and unrelated to other disorders (American Academy of Sleep Medicine, 2014; Robert and Zadra, 2014). Their content is unspecific and includes interpersonal conflict, failure, helplessness, apprehension, being chased, accident, evil force, disaster, and environmental abnormality (Mota-Rolim et al., 2013). According to the “threat simulation theory,” nightmares serve adaptation to stressful events in life (Revonsuo, 2000). However, recent observations point to maladaptive effects of nightmares on sleep and daytime neurobehavioral functions (Levin and Nielsen, 2007; American Academy of Sleep Medicine, 2014; Scarpelli et al., 2019). In contrast, posttraumatic nightmares refer to dreaming disturbances that are part of the stress reaction following exposure to a traumatic event, either during the acute stress response, or over the course of PTSD. Whereas approximately 2–8% of the general population suffers from idiopathic nightmares, nightmares are a core feature of PTSD, with up to 80% of individuals with PTSD reporting disturbing and suicidal dreams with some degree of resemblance to the actual traumatic event (Hasler and Germain, 2009; American Academy of Sleep Medicine, 2014).
Regarding anxiety disorder, it has been found that whereas stress increases frequencies of negative emotions in dreams and nightmares occurrence (Lauer et al., 1987; de Koninck and Brunette, 1991; Köthe and Pietrowsky, 2001), nightmares in turn increase anxiety (Schredl, 2003; Scarpelli et al., 2019). Levin and Fireman (2002) found that in a long run, the reported distress associated with nightmare experience impacted more negatively on quality of life than their frequency did. This finding appears to significantly challenge the “threat simulation theory” (Revonsuo, 2000). It is important to note that whereas nightmare frequency is the number of occurrences of the nightmare, nightmare distress refers to the negative feelings upon awakening following nightmare (Belicki, 1992; Blagrove et al., 2004). In depressed patients, there is a relationship between nightmares and suicides (Agargun et al., 1998; Agargun and Cartwright, 2003; Bernert et al., 2005; Sjöström et al., 2007). The bad feeling soon after awaking from nightmares persists during the rest of the day, being associated with a melancholy and increased suicide risk (Agargun et al., 2007).
The etiology of nightmares is still elusive (Gieselmann et al., 2019). According to the neurocognitive theory, dreams are not mainly generated by the brainstem REMS control, but rather by complex forebrain mechanisms independently of the REMS state (Solms, 2000). According to the impaired fear extinction model (Germain et al., 2008; Nielsen and Levin, 2007), a process of recombining fearful memories with novel and dissociated contexts is continuously activated in nightmare disorder. As stipulated by the affect network dysfunction model (Nielsen and Levin, 2007), individuals high in affect load and affect distress are particularly prone to such impaired fear extinction. In addition, this model is proposed in the trait susceptibility theory of nightmares, which suggests that individuals with frequent nightmares display an increased depth of processing of both negative and positive semantic stimuli (Carr et al., 2016). Finally, all the above factors may contribute to the condensing of recurrent nightmare elements into a nightmare script (Spoormaker, 2008).
Idiopathic nightmares and those related to PTSD, anxiety, depression and other disorders can be treated with lucid dreaming therapy (LDT). Lucid dreams (LD) are those in which the subjects are aware that they are dreaming during the dream, and even may control the oneiric plot (LaBerge, 1980; Mota-Rolim and Araujo, 2013; Baird et al., 2019). This possibility opens a way to help the bearers of nightmares from what is known as re-signification of the dream scene: Being lucid in a nightmare, one can stop fearing the threats by knowing that it is only a dream, and that it could never bring real physical damage. Another tactic would be to face the source of fear, such as monsters, for example (Saint-Denys, 1982), or talk to these monsters in an attempt to find out if they have any specific reason for being there (Tholey, 1988). According to Mota-Rolim and Araujo (2013), individuals can also wake up during the nightmare, try to neutralize it, or even make it enjoyable. Here we would like to answer three basic questions: (1) Is LDT effective for treating nightmares? (2) What are the mechanisms by which LDT works? (3) What are the most used procedures, and the limitations of the LDT?
Materials and Methods
We searched for original research articles in scientific databases, such as PubMed, Medline, PsycINFO, Web of Science, and Scopus using the keywords “lucid dream(s)” or “lucid dreaming” and “nightmare(s)” or “recurrent nightmare.” Our inclusion criteria were: (1) original research articles; (2) written in English; (3) investigated LDT for nightmares. Our exclusion criteria were: (1) original findings replicated in books, book chapters and reviews; (2) purposed on for issues different from clinical use of LDT for recurring nightmares (Figure 1). Data was extracted by three researchers and then reviewed by three (including one that extracted data as well).
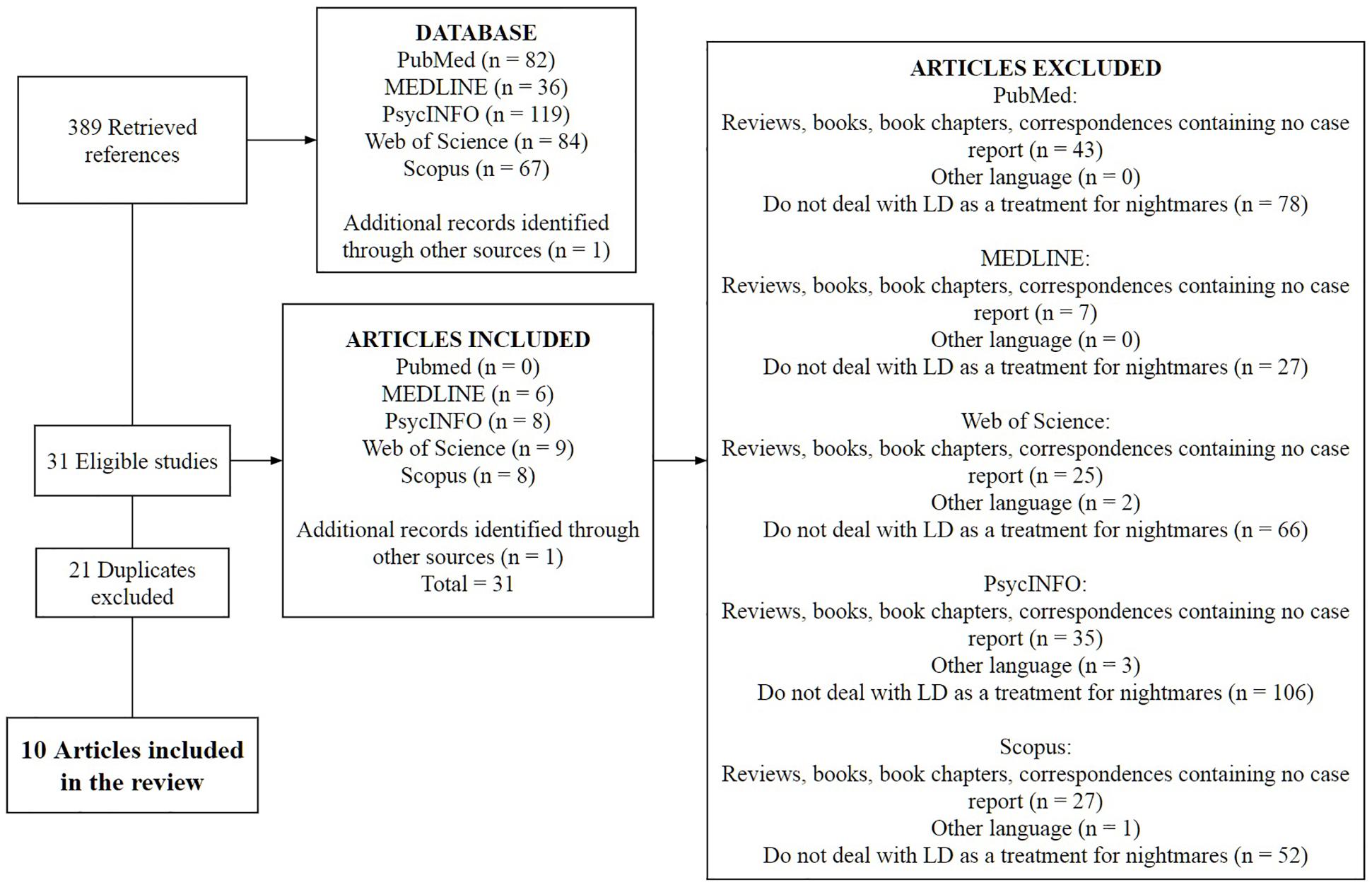
Figure 1. Flowchart showing the screening of the articles that deal with LD as a treatment for recurrent nightmares.
Results
We found 10 original research articles dealing with LDT as a therapeutic approach for nightmares (Table 1). Five case report studies demonstrated beneficial effects of LDT on nightmares and related distress (Halliday, 1982; Brylowski, 1990; Abramovitch, 1995; Tanner, 2004; Been and Garg, 2010). However, case reports cannot prove statistically the beneficial effect of LDT on nightmare frequency, associated distress and worsened sleep quality. Further, several cross-sectional and randomized studies reported for effects of LDT and other psychotherapeutic approaches used to induce LD in order to alleviate basic features of nightmares. Zadra and Pihl (1997) applied long-lasting progressive muscle relaxation and imagery rehearsal therapy (IRT), as a cue for induction of LD in a small sample of recurrent nightmare sufferers. They showed some positive but insignificant effects on nightmare features. Spoormaker et al. (2003) found a positive but also not significant effect of LDT on nightmare frequency and sleep quality. Spoormaker and van den Bout (2006) demonstrated that participants who received individual LDT showed a stronger decrease in nightmare frequency compared to the group that received LDT. Lancee et al. (2010) subjected a larger group of volunteers with self-reported nightmares to IRT, IRT with sleep hygiene and IRT with sleep hygiene and a LD session. They found that application of IRT only was more effective than the other interventions. More recently, Holzinger et al. (2015) subjected participants who suffered from frequent nightmares, and who did not make use of any medication to gestalt therapy (GT) and a combination of GT and LDT. The major results from this randomized study showed that the group that received GT plus LDT had better effects on nightmare features than those subjected to GT only (Table 1).
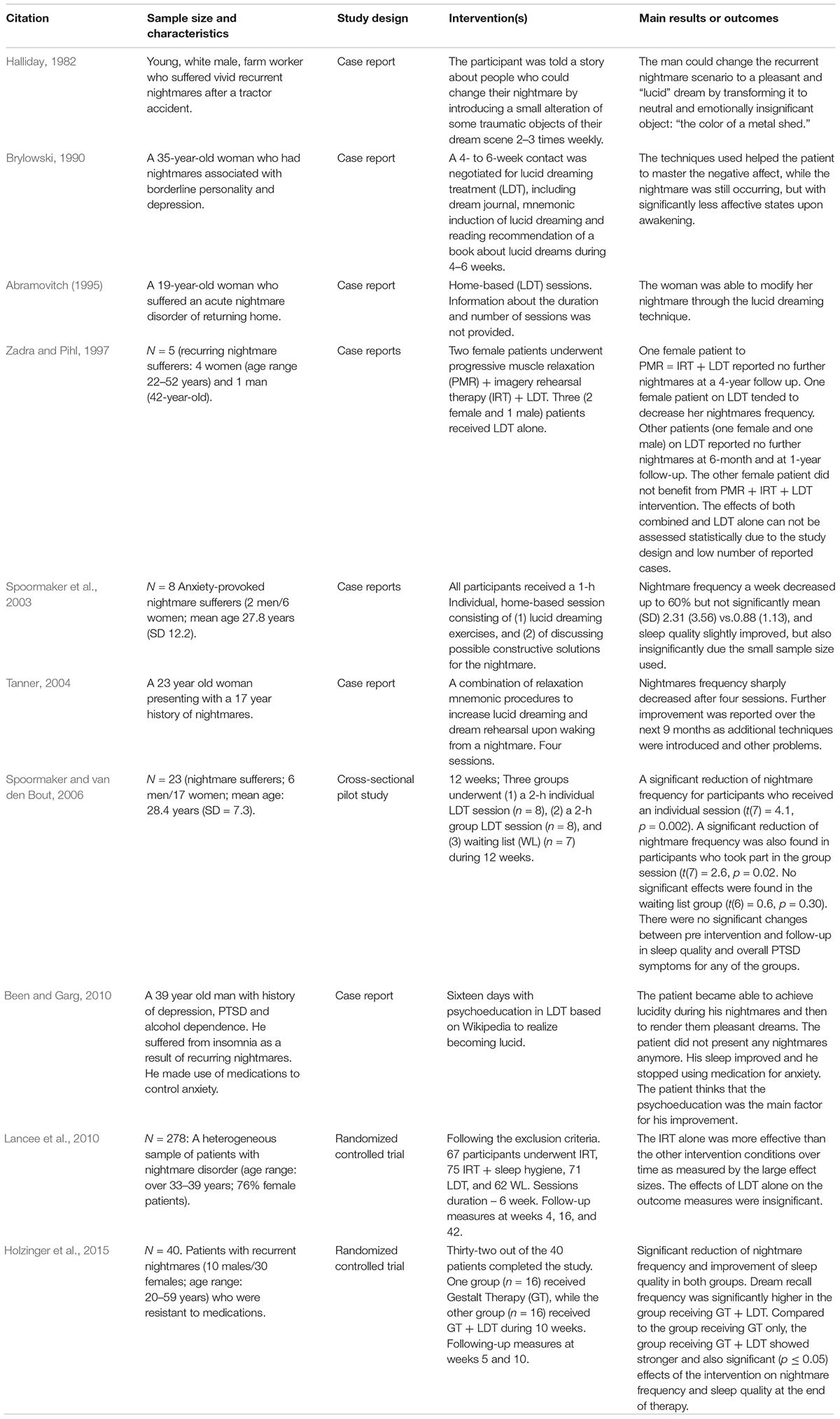
Table 1. Summary of the included studies details.
Discussion
What Are the Neurobiological and Psychological Mechanisms That Underlie LDT?
At the neurobiological level, LDT may work by frontal activation, which inhibits the limbic system. During normal REMS, the frontal activity decreases (Maquet et al., 1996); however, during LD the frontal gamma activity (∼40 Hz) increases (Mota-Rolim et al., 2008, 2010; Voss et al., 2009). The frontal region is associated with executive control, attention, rational judgment, working memory, etc. (Hobson, 2009), while the limbic system is related to emotional processes (Peterson et al., 2002). During REMS, there is also an increase in dopamine levels in limbic areas, mainly the nucleus accumbens (Joyce and Meador-Woodruff, 1997; Gottesmann, 2006; McCarley, 2007; Skrzypińska and Szmigielska, 2013). This neurotransmitter pattern and brain areas activity observed in non-lucid REMS are similar to those involved in psychosis (Tort et al., 2005), which may explain the bizarre aspect of dreams (which are analogous to hallucinations), and the lack of rational judgment over this bizarreness (akin the delirious thinking) (Mota et al., 2016). Thus, suppression of the limbic system by the frontal lobe activation during LD could decrease both frequency and intensity of nightmares. Finally, Dresler et al. (2012) observed that the precuneus region is linked to the first-person perspective and agency during LD, which is an important aspect for the treatment of nightmares.
At the psychological level, Rousseau and Belleville (2017) gathers possible mechanisms by which LDT and other similar treatments work, which are: modification of beliefs (Krakow et al., 2000), prevention of avoidance (Pruiksma, 2012), decreased arousal (Davis, 2009), restoration of sleep functions (Germain, 2002), emotional processing (Davis et al., 2007), and sense of mastery (Spoormaker et al., 2003). Change in beliefs can happen both through psychoeducation about the aspects of dreams (Krakow, 2015) and through psychotherapy, focusing on the nightmare theme (Harb et al., 2012). In the case reported by Been and Garg (2010), for example, the patient believes that the psychoeducation was the main factor for his improvement. Avoidance, i.e., trying not to think about the nightmare content or avoiding sleep, is associated with nightmare maintenance (Hansen et al., 2013), and being afraid to fall asleep correlates with higher nightmare frequency (Neylan et al., 1998). Relaxation exercises, as well the sense of mastery itself could help to decrease arousal (Rousseau and Belleville, 2017). Once nightmares are diminished, the subject awakes less, which allows the restoration of sleep functions such as memory consolidation and emotional processing (Germain, 2002). Finally, the belief in control, i.e., the sense of mastery, seems equally important as actually controlling the dream (Spoormaker et al., 2003). Harb et al. (2016) compared the cognitive-behavioral therapy for insomnia (cCBT-I) with IRT + cCBT-I to investigate the potential role of LD as a mechanism of action of IRT in military veterans with PTSD and recurrent nightmares. Before treatment, veterans demonstrated a LD profile characterized by high dream awareness and low dream content control. Following treatment, the control of dream content increased, but lucidity has not changed. This increase in dream content control was related to a reduction in nightmare distress.
Studies show that lucidity is not the main factor to change nightmare content or to reduce nightmare frequency (Spoormaker and van den Bout, 2006). Therefore, a relevant question is: what are the advantages of using LDT over other therapies, e.g., IRT? First, even though lucidity is not the main factor, it does not mean it has no important role. The possibility to achieve lucidity may provide the opportunity to practice self-control and pacific confrontation more directly, which is important to improve the coping ability in the waking state (Brylowski, 1990). According to Lancee et al. (2010), there are two main advantages of LDT over other therapies, especially IRT: (a) once LDT targets the nightmare within the dream, it might be specifically beneficial for people that suffer from non-recurrent nightmares; (b) LDT has more effect on nightmare intensity, because nightmare sufferers achieve a sense of control with the LD technique. Moreover, unlike LDT, IRT might only ameliorate the low intensity nightmares (Lancee et al., 2010). As another advantage, even without lucidity, LDT encourages the attitude of “this is just a nightmare, so there is no real threat.” Although IRT also helps to deal with negative imagery (Krakow and Zadra, 2006), the attitude of “this is just a dream” may play an important role in the modification of belief, decrease of arousal and prevention of avoidance (see Supplementary Material). Despite that, more studies are needed to clarify the mechanisms of therapies that aim to treat nightmares, and to indicate their advantages and disadvantages.
How Does LDT Work on Practice?
Lucid dreaming therapy for nightmares is a focal modality of psychotherapy. It can happen in a 6-week period (Brylowski, 1990), but can produce effects in a single session (Zadra and Pihl, 1997). The first step is to make it clear that patients have the full capacity to learn how to control their dreams. The therapist guides patients to develop LD induction techniques, and help them to deal with the fear that can follow LD discovery. Once patients feel empowered about their dreams, nightmare frequency might decrease by itself (Spoormaker and van den Bout, 2006). Beyond that, if a nightmare comes up, it will tend to be less distressing, given the sense of mastery that the patient now has. The experience of facing the oneiric threat, i.e., of having a less distressing dream, seems to be essential to the decrease of the remaining nightmares.
Further, a long-term psychotherapy may be initiated, aiming to explore more profoundly the waking life and to elucidate broader questions that even may trigger the nightmares. LDT is a good precedent of a long-term psychotherapy, once it has relatively quick results, which motivates the patient to continue in therapy (Holzinger et al., 2015). Some patients may be skeptic, may have more difficulty to achieve lucidity, or may just have no time to practice frequently at home. In these cases, we recommend using techniques of external sensory stimulation during REMS or substances to induce LD more quickly (Stumbrys et al., 2012; Baird et al., 2019; Mota-Rolim et al., 2019). Nevertheless, some studies demonstrate that even when lucidity is not achieved, exercises of induction facilitates waking up from the nightmare before it becomes too scary (Brylowski, 1990; Tanner, 2004), or changes the oneiric content even without lucidity (Spoormaker and van den Bout, 2006). In these cases, the subjects incorporated elements from the exercises into the dream (Brylowski, 1990; Zadra and Pihl, 1997; Spoormaker et al., 2003). Thus, such exercises helped patients to increase the sense of control over their dreams, consequently, increasing their self-confidence. Moreover, the positive changes in the threatening content are symbolically incorporated to the dreamer’s cognition (Brylowski, 1990).
As said earlier, wake up through lucidity is an option to reduce distress related to nightmares. However, LaBerge and Rheingold (1990) believe that “just wake up” is not as therapeutic as to actually control the content of the dream or the self, once it is a way to run from the nightmare, and not to face it. These authors even suggest that controlling the self is better than controlling the dream content, since in real life, it is not possible to magically change the scenario. Tholey (1988) affirms that when the dream ego looks courageously and openly at hostile dream figures, their appearance often becomes less threatening, as recently supported by Stumbrys and Erlacher (2017) empirical study. On the other hand, when one tries to make a dream figure disappear, it may become even more threatening (Sparrow, 1976). Finally, Tholey (1988) also argue that it is better to conciliate with the dream figure through constructive dialogue than to attack it. Although emotions such as intense fear can trigger lucidity faster (LaBerge and Rheingold, 1990), an unexperienced lucid dreamer is more prone to wake up from the dream than trying to control it, since the excitement caused by the discovery that one is dreaming may cause awakening (Mota-Rolim et al., 2013). Besides, even when subjects are lucid, the fear may not necessarily fade away (Hurd, 2014), thus a “runaway” behavior takes place. Initially, “just wake up” could be a useful weapon until a minimum sense of control is developed; however, it is necessary to practice for the LD scenario does not fade away causing the awakening, which allows the dreamer to explore other possibilities and face their fears.
What Are the Main Limitations of the LDT?
Halliday (1988) and Zadra (1990) reported case studies in which lucidity was achieved, but without control, and it actually worsened the nightmare. Lucid nightmares are LD with a scary and unpleasant content, in which dreamers have no control over the situation, thus they just “witness” the unfolding of the dream, being unable to deliberately wake up (Hurd, 2009; Schredl and Göritz, 2018; Stumbrys, 2018). Lucid nightmares may be even more terrifying than common nightmares (Halliday, 1988); however, Stumbrys (2018) found that the levels of nightmare vs. lucid nightmare distress do not differ. Sparrow (1991), signifying dreamer’s harrowing experiences with LD, warned about the wholesale advertising of LD, since lucid nightmares frequency is associated not only to nightmare frequency, but also to LD frequency (Stumbrys, 2018). This makes patients with nightmares very vulnerable to lucid nightmares in a LDT. Therefore, some care is needed when a LDT is initiated. Fortunately, community support is helpful in reducing lucid nightmares (Hurd, 2006). Besides, it was found that dopamine agonists are useful in reducing lucid nightmares frequency (McLaughlin et al., 2015a, b, 2016); however, these studies comprise only a few cases in a very special population, which limits the generalizability of the findings. Finally, one main issue in LDT is to induce LD, which is usually difficult for most of people (Stumbrys et al., 2012), who experience LD rarely (Mota-Rolim et al., 2013). However, Dodet et al. (2015) and Rak et al. (2015) observed that narcoleptic patients report more LD than the rest of population, and that some of these patients even learned to use LD to change their recurrent nightmares. These authors suggest that the experience of these patients with LD could help other narcoleptics who suffer from frequent nightmares.
Conclusion
Lucid dreaming therapy may be efficient for treating nightmares, and even when lucidity is not achieved, the induction exercises assisted patients by helping them develop a critical thinking over dream content. Although induction of LD may be a feasible aid in the treatment of patients with nightmares through minimizing their frequency, intensity and psychological distress, the available literature is still scarce and does not provide consistent results. Furthermore, the samples size are limited, which precludes more significant comparisons. Therefore, more research is clearly warranted for a better estimation of the effective conductance and therapeutic outcome of LD techniques in clinical practice.
Author Contributions
TM and RK conducted the literature search, selected the eligible studies, and drafted the manuscript. GF drafted the manuscript. KA selected the eligible studies and drafted the manuscript. SM-R designed the manuscript, conducted the literature search, selected the eligible studies, and drafted the manuscript. All authors worked over the first draft of the manuscript and approved the final version.
Funding
TM, GF, KA, and SM-R were supported by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES), Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq), Financiadora de Estudos e Projetos do Ministério da Ciência e Tecnologia (FINEP), and Fundação de Apoio à Pesquisa do Estado do Rio Grande do Norte (FAPERN). RK was supported by the Foundation for Scientific Research of the Bulgarian Academy of Sciences.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyg.2019.02618/full#supplementary-material
References
Abramovitch, H. (1995). The nightmare of returning home: a case of acute onset nightmare disorder treated by lucid dreaming. Isr. J. Psychiatry Relat. Sci. 32, 140–145.
Agargun, M. Y., Besiroglu, L., Cilli, A. S., Gulec, M., Aydin, A., Inci, R., et al. (2007). Nightmares, suicide attempts, and melancholic features in patients with unipolar major depression. J. Affect Disord. 98, 267–270. doi: 10.1016/j.jad.2006.08.005
Agargun, M. Y., and Cartwright, R. (2003). REM sleep, dream variables and suicidality in depressed patients. Psychiatry Res. 119, 33–39. doi: 10.1016/s0165-1781(03)00111-2
Agargun, M. Y., Cilli, A. S., Kara, H., Tarhan, N., Kincir, F., and Oz, H. (1998). Repetitive and frightening dreams and suicidal behavior in patients with major depression. Compr. Psychiatry 39, 198–202. doi: 10.1016/s0010-440x(98)90060-8
American Academy of Sleep Medicine (2014). International Classification of Sleep Disorders, 3rd Edn. Darien, IL: American Academy of Sleep Medicine.
Aurora, R. N., Zak, R. S., Auerbach, S. H., Casey, K. R., Chowdhuri, S., Karippot, A., et al. (2010). Best practice guide for the treatment of nightmare disorder in adults. J. Clin. Sleep Med. 6, 389–401.
Baird, B., Mota-Rolim, S. A., and Dresler, M. (2019). The cognitive neuroscience of lucid dreaming. Neurosci. Biobehav. Rev. 100, 305–323. doi: 10.1016/j.neubiorev.2019.03.008
Been, G., and Garg, V. (2010). Nightmares in the context of PTSD treated with psychoeducation regarding lucid dreaming. Aust. N. Z. J. Psychiatry 44:583. doi: 10.1080/00048671003614213
Belicki, K. (1992). Nightmare frequency versus nightmare distress: relations to psychopathology and cognitive style. J. Abnorm. Psychol. 101, 592–597. doi: 10.1037/0021-843x.101.3.592
Bernert, R. A., Joiner, T. E. Jr., Cukrowicz, K. C., Schmidt, N. B., and Krakow, B. (2005). Suicidality and sleep disturbances. Sleep 28, 1135–1141. doi: 10.1093/sleep/28.9.1135
Blagrove, M., Farmer, L., and Williams, E. (2004). The relationship of nightmare frequency and nightmare distress to well-being. J. Sleep Res. 13, 129–136. doi: 10.1111/j.1365-2869.2004.00394.x
Brylowski, A. (1990). Nightmares in crisis: clinical applications of lucid dreaming techniques. Psychiatr. J. Univ. Ott. 15, 79–84.
Carr, M., Blanchette-Carrière, C., Marquis, L. P., Ting, C., and Nielsen, T. (2016). Nightmare sufferers show atypical emotional semantic breadth and prolonged REM sleep-dependent emotional priming. Sleep Med Rev. 20, 80–87. doi: 10.1016/j.sleep.2015.11.013
Davis, J. L. (2009). Treating Post-Trauma Nightmares: A Cognitive Behavioral Approach. New York, NY: Springer Publishing Co.
Davis, J. L., Byrd, P., Rhudy, J. L., and Wright, D. C. (2007). Characteristics of chronic nightmares in a trauma-exposed treatment-seeking sample. Dreaming 17, 187–198. doi: 10.1037/1053-0797.17.4.187
de Koninck, J., and Brunette, R. (1991). Presleep suggestion related to a phobic object: successful manipulation of reported dream affect. J. Gen. Psychol. 118, 185–200. doi: 10.1080/00221309.1991.9917780
Saint-Denys, H. de. (1982). “Dreams and the Means of Directing Them,” in From the French Les Reves et Les Moyens de Les Diriger (1867). Paris: Amyat, ed. M. Schatzman. Trans. N. Fry, (London: Duckworth).
Dodet, P., Chavez, M., Leu-Semenescu, S., Golmard, J. L., and Arnulf, I. (2015). Lucid dreaming in narcolepsy. Sleep 38, 487–497. doi: 10.5665/sleep.4516
Dresler, M., Wehrle, R., Spoormaker, V. I., Koch, S. P., Holsboer, F., Steiger, A., et al. (2012). Neural correlates of dream lucidity obtained from contrasting lucid versus non-lucid REM sleep: a combined EEG/fMRI case study. Sleep 35, 1017–1020. doi: 10.5665/sleep.1974
Germain, A. (2002). Sleep Pathophysiology and Cognitive-Behavioral Treatment of Posttraumatic and Idiopathic Nightmares. Ann Arbor, MI: PQIL.
Germain, A., Buysse, D. J., and Nofzinger, E. A. (2008). Sleep – specific mechanisms underlying posttraumatic stress disorder: integrative review and neurobiological hypotheses. Sleep Med Rev. 12, 185–195. doi: 10.1016/j.smrv.2007.09.003
Germain, A., and Nielsen, T. A. (2003). Sleep pathophysiology in posttraumatic stress disorder and idiopathic nightmare sufferers. Biol. Psychiatry. 54, 1092–1098. doi: 10.1016/s0006-3223(03)00071-4
Gieselmann, A., Ait Aoudia, M., Carr, M., Germain, A., Gorzka, R., Holzinger, B., et al. (2019). Aetiology and treatment of nightmare disorder: state of the art and future perspectives. J. Sleep Res. 28:e12820. doi: 10.1111/jsr.12820
Gottesmann, C. (2006). The dream sleeping stage: a new neurobiological model schizophrenia? Neuroscience 140, 1105–1115. doi: 10.1016/j.neuroscience.2006.02.082
Halliday, G. (1982). Direct alteration of a traumatic nightmare. Percep. Mot. Skills 54, 413–414. doi: 10.2466/pms.1982.54.2.413
Halliday, G. (1988). “Lucid dreaming: use in nightmares and sleep-wake confusion,” In Conscious Mind, Sleeping Brain, (Eds.) J. Gackenbach, and S. LaBerge, (New York, NY: Plenum Press), 306.
Hansen, K., Höfling, V., Kröner-Borowik, T., Stangier, U., and Steil, R. (2013). Efficacy of psychological interventions aiming to reduce chronic nightmares: a meta-analysis. Clin. Psychol. Rev. 33, 146–155. doi: 10.1016/j.cpr.2012.10.012
Harb, G. C., Brownlow, J. A., and Ross, R. J. (2016). Posttraumatic nightmares and imagery rehearsal: the possible role of lucid dreaming. Dreaming 26, 238–249. doi: 10.1037/drm0000030
Harb, G. C., Thompson, R., Ross, R. J., and Cook, J. M. (2012). Combat-related PTSD nightmares and imagery rehearsal: nightmare characteristics and relation to treatment outcome. J. Trauma Stress 25, 511–518. doi: 10.1002/jts.21748
Hartmann, E. (1984). The Nightmare: The Psychology and Biology of Terrifying Dreams. New York, NY: Basic Books, 294.
Hasler, B., and Germain, A. (2009). Correlates and treatments of nightmares in adults. Sleep Med. Clin. 4, 507–517. doi: 10.1016/j.jsmc.2009.07.012
Haynes, S. N., and Mooney, D. K. (1975). Nightmares: etiological, theoretical, and behavioral treatment considerations. Psychol. Rec. 25, 225–236. doi: 10.1007/BF03394308
Hobson, A. (2009). The neurobiology of consciousness: lucid dreaming wakes up. Int. J. Dream Res. 2, 41–44. doi: 10.11588/ijodr.2009.2.403
Holzinger, B., Klösch, G., and Saletu, B. (2015). Studies with lucid dreaming as add-on therapy to gestalt therapy. Acta Neurol. Scand. 131, 355–363. doi: 10.1111/ane.12362
Hurd, R. (2006). “Lucid dreaming: new perspectives of consciousness in sleep,” in Proceedings of the Presentation at “The Transformative Power of Dream Studies” Panel, the Annual Conference of the International Association for the Study of Dreams, (Bridgewater, MA).
Hurd, R. (2009). “Lucid nightmares: the dark side of self-awareness in dreams,” in Proceedings of the Annual Conference of the International Association for the Study of Dreams, (Chicago, IL).
Hurd, R. (2014). ““Unearthing the Paleolithic Mind in Lucid Dreams,” in Lucid Dreaming: New Perspectives on Consciousness, eds R. Hurd and K. Bulkeley, (Santa Barbara, CA: ABC-CLIO), 277–324.
Joyce, J. N., and Meador-Woodruff, J. H. (1997). Linking the family of D2 receptors to neuronal circuits in human brain: insights into schizophrenia. Neuropsychopharmacology 16, 375–384. doi: 10.1016/s0893-133x(96)00276-x
Köthe, M., and Pietrowsky, R. (2001). Behavioral effects of nightmares and their correlations to personality patterns. Dreaming 11, 43–52. doi: 10.1023/A:1009468517557
Krakow, B. (2015). “Nightmare therapy: emerging concepts from sleep medicine,” in Dream Research: Contributions to Clinical Practice, ed. M. K. M. Glucksman, (New York, NY: Routledge/Taylor & Francis Group), 149–160.
Krakow, B., Hollifield, M., Schrader, R., Koss, M., Tandberg, D., Lauriello, J., et al. (2000). A controlled study of imagery rehearsal for chronic nightmares in sexual assault survivors with PTSD: a preliminary report. J. Trauma Stress 13, 589–609. doi: 10.1023/a:1007854015481
Krakow, B., and Zadra, A. (2006). Clinical management of chronic nightmares: imagery rehearsal therapy. Behav. Sleep Med. 4, 45–70. doi: 10.1207/s15402010bsm0401_4
LaBerge, S. (1980). Lucid dreaming as a learnable skill: a case study. Percept. Motor Skills 51, 1039–1042. doi: 10.2466/pms.1980.51.3f.1039
LaBerge, S., and Rheingold, H. (1990). Exploring the World of Lucid Dreaming. New York, NY: Ballantine Books.
Lancee, J., van den Bout, J., and Spoormaker, V. I. (2010). Expanding self-help imagery rehearsal therapy for nightmares with sleep hygiene and lucid dreaming: a waiting-list controlled trial. Int. J. Dream Res. 3, 111–120. doi: 10.11588/ijodr.2010.2.6128
Lauer, C., Riemann, D., Lund, R., and Berger, M. (1987). Shortened REM latency: a consequence of psychological strain? Psychophysiology 24, 263–271. doi: 10.1111/j.1469-8986.1987.tb00293.x
Levin, R. (1998). Nightmares and schizotypy. Psychiatry 61, 206–216. doi: 10.1080/00332747.1998.11024832
Levin, R., and Fireman, G. (2002). Nightmare prevalence, nightmare distress, and self-reported psychological disturbance. Sleep 25, 205–212.
Levin, R., and Nielsen, T. A. (2007). Disturbed dreaming, posttraumatic stress disorder, and affect distress: a review and neurocognitive model. Psychol. Bull. 133, 482–528. doi: 10.1037/0033-2909.133.3.482
Maquet, P., Péters, J.-M., Aerts, J., Delfiore, G., Degueldre, C., Luxen, A., et al. (1996). Functional neuroanatomy of human rapid-eye-movement sleep and dreaming. Nature 383, 163–166. doi: 10.1038/383163a0
McCarley, R. W. (2007). Neurobiology of REM and NREM sleep. Sleep Med. 8, 302–330. doi: 10.1016/j.sleep.2007.03.005
McLaughlin, T., Blum, K., Oscar-Berman, M., Febo, M., Agan, G., Fratantonio, J. L., et al. (2015a). Putative dopamine agonist (KB220Z) attenuates lucid nightmares in PTSD patients: role of enhanced brain reward functional connectivity and homeostasis redeeming joy. J. Behav. Addict. 4, 106–115. doi: 10.1556/2006.4.2015.008
McLaughlin, T., Blum, K., Oscar-Berman, M., Febo, M., Demetrovics, Z., Agan, G., et al. (2015b). Using the neuroadaptagen KB200zTM to ameliorate terrifying, lucid nightmares in RDS patients: the role of enhanced, brain-reward, functional connectivity and dopaminergic homeostasis. J. Reward Defic. Syndr. 1, 24–35. doi: 10.17756/jrds.2015-006
McLaughlin, T., Febo, M., Badgaiyan, R. D., Barh, D., Dushaj, K., Braverman, E. R., et al. (2016). KB220ZTM a pro-dopamine regulator associated with the protracted, alleviation of terrifying lucid dreams. Can we infer neuroplasticity-induced changes in the reward circuit? J. Reward Defic. Syndr. Addict. Sci. 2, 3–13. doi: 10.17756/jrdsas.2016-022
Morgenthaler, T. I., Auerbach, S., Casey, K. R., Kristo, D., and Maganti, R. (2018). Position paper for the treatment of nightmare disorder in adults: an american academy of sleep medicine position paper. J. Clin. Sleep Med. 14, 1041–1055. doi: 10.5664/jcsm.7178
Mota, N. B., Resende, A., Mota-Rolim, S. A., Copelli, M., and Ribeiro, S. (2016). Psychosis and the control of lucid dreaming. Front. Psychol. 7:294. doi: 10.3389/fpsyg.2016.00294
Mota-Rolim, S., Pantoja, A., Pinheiro, R., Camilo, A., Barbosa, T., Hazboun, I., et al. (2008). “Lucid dream: sleep electroencephalographic features and behavioral induction methods,” in First Congress IBRO/LARC of Neurosciences for Latin America, Caribbean and Iberian Peninsula, (Búzios).
Mota-Rolim, S. A., and Araujo, J. F. (2013). Neurobiology and clinical implications of lucid dreaming. Med. Hypotheses 81, 751–756. doi: 10.1016/j.mehy.2013.04.049
Mota-Rolim, S. A., Erlacher, D., Tort, A. B. L., Araujo, J. F., and Ribeiro, S. (2010). Different kinds of subjective experience during lucid dreaming may have different neural substrates. Int. J. Dream Res. 3, 33–35. doi: 10.11588/ijodr.2010.1.596
Mota-Rolim, S. A., Pavlou, A., Nascimento, G., Araujo, J. F., and Ribeiro, S. (2019). Portable devices to induce lucid dreams – are they reliable? Front. Neurosci. 13:428. doi: 10.3389/fnins.2019.00428
Mota-Rolim, S. A., Targino, Z. H., Souza, B. C., Blanco, W., Araujo, J. F., and Ribeiro, S. (2013). Dream characteristics in a Brazilian sample: an online survey focusing on lucid dreaming. Front. Hum. Neurosci. 7:836. doi: 10.3389/fnhum.2013.00836
Neylan, T. C., Marmar, C. R., Metzler, T. J., Weiss, D. S., Zatzick, D. F., Delucchi, K. L., et al. (1998). Sleep disturbances in the vietnam generation: findings from a nationally representative sample of male vietnam veterans. Am. J. Psychiatry 155, 929–933. doi: 10.1176/ajp.155.7.929
Nielsen, T., and Levin, R. (2007). Nightmares: a new neurocognitive model. Sleep Med. Rev. 11, 295–310. doi: 10.1016/j.smrv.2007.03.004
Nielsen, T. A., LaBerge, L., Paquet, J., Tremblay, R. E., Vitaro, F., Montplaisir, J., et al. (2000). Development of disturbing dreams during adolescence and their relation to anxiety symptoms. Sleep 23, 727–736.
Peterson, N. D. J., Henke, P. G., and Hayes, Z. (2002). Limbic system function and dream content in university students. J. Neuropsychiatry Clin. Neurosci. 14, 283–288. doi: 10.1176/appi.neuropsych.14.3.283
Pruiksma, K. M. E. (2012). A Randomized Controlled Trial of Exposure, Relaxation, and Rescripting Therapy and Relaxation Training for Chronic Nightmares in Trauma-Exposed Persons: Findings at one Week Posttreatment. Tulsa, OK: University of Tulsa.
Rak, M., Beitinger, P., Steiger, A., Schredl, M., and Dresler, M. (2015). Increased lucid dreaming frequency in narcolepsy. Sleep 38, 787–792. doi: 10.5665/sleep.4676
Revonsuo, A. (2000). The reinterpretation of dreams: an evolutionary hypothesis of the function of dreaming. Behav. Brain Sci. 23, 877–901. doi: 10.1017/s0140525x00004015
Robert, G., and Zadra, A. (2014). Thematic and content analysis of idiopathic nightmares and bad dreams. Sleep 37, 409–417. doi: 10.5665/sleep.3426
Rousseau, A., and Belleville, G. (2017). The mechanisms of action underlying the efficacy of psychological nightmare treatments: a systematic review and thematic analysis of discussed hypotheses. Sleep Med. Rev. 39, 122–133. doi: 10.1016/j.smrv.2017.08.004
Scarpelli, S., Bartolacci, C., D’Atri, A., Gorgoni, M., and De Gennaro, L. (2019). The functional role of dreaming in emotional processes. Front. Psychol. 10:459. doi: 10.3389/fpsyg.2019.00459
Schredl, M. (2003). Effects of state and trait factors on nightmare frequency. Eur. Arch. Psychiatry Clin. Neurosci. 253, 241–247. doi: 10.1007/s00406-003-0438-1
Schredl, M., and Göritz, A. S. (2018). Nightmare themes: an online study of most recent nightmares and childhood nightmares. J. Clin. Sleep Med. 14, 465–471. doi: 10.5664/jcsm.7002
Sjöström, N., Wærn, M., and Hetta, J. (2007). Nightmares and sleep disturbances in relation to suicidality in suicide attempters. Sleep 30, 91–95. doi: 10.1093/sleep/30.1.91
Skrzypińska, D., and Szmigielska, B. (2013). What links schizophrenia and dreaming? Common phenomenological and neurobiological features of schizophrenia and REM sleep. Arch. Psychiatry Psychother. 2, 29–35. doi: 10.12740/app/18443
Solms, M. (2000). Dreaming and REM sleep are controlled by different brain mechanisms. Behav. Brain Sci. 23, 843–850. doi: 10.1017/s0140525x00003988
Sparrow, G. S. (1976). Lucid Dreaming: Dawning of the Clear Light. Virginia Beach, VA: A. R. E. Press, 33.
Spoormaker, V. I., Van De Bout, J., and Meijer, E. J. G. (2003). Lucid dreaming treatment for nightmares: a series of cases. Dreaming 13, 181–186. doi: 10.1037/1053-0797.13.3.181
Spoormaker, V. I., and van den Bout, J. (2006). Lucid dreaming treatment for nightmares: a pilot study. Psychother. Psychosom. 75, 389–394. doi: 10.1159/000095446
Stumbrys, T. (2018). Lucid nightmares: a survey of their frequency, features, and factors in lucid dreamers. Dreaming 28, 193–204. doi: 10.1037/drm0000090
Stumbrys, T., and Erlacher, D. (2017). Inner ghosts: encounters with threatening dream characters in lucid dreams. Dreaming 27, 40–48. doi: 10.1037/drm0000043
Stumbrys, T., Erlacher, D., Schadlich, M., and Schredl, M. (2012). Induction of lucid dreams: a systematic review of evidence. Conscious. Cogn. 21, 1456–1475. doi: 10.1016/j.concog.2012.07.003
Tanner, B. (2004). Multimodal behavioral treatment of nonrepetitive, treatment-resistant nightmares: a case report. Percept. Mot. Skills 99, 1139–1146. doi: 10.2466/pms.99.3f.1139-1146
Tanskanen, A., Tuomilehto, J., Viinamaki, H., Vartiainen, E., Lehtonen, J., and Puska, P. (2001). Nightmares as predictors of suicide. Sleep 24, 845–848.
Tholey, P. (1988). “A model for lucidity training as a means of self-healing and psychological growth,” in Conscious Mind, Sleeping Brain: Perspectives on Lucid Dreaming, eds J. Gackenbach and S. LaBerge, (New York, NY: Plenum), 265.
Tort, A. B., Dall’Igna, O. P., de Oliveira, R. V., Mantese, C. E., Fett, P., Gomes, M. W., et al. (2005). Atypical antipsychotic profile of flunarizine in animal models. Psychopharmacology 177, 344–348. doi: 10.1007/s00213-004-1955-y
Voss, U., Holzmann, R., Tuin, I., and Hobson, J. A. (2009). Lucid dreaming: a state of consciousness with features of both waking and non-lucid dreaming. Sleep 32, 1191–1200. doi: 10.1093/sleep/32.9.1191
Zadra, A., and Donderi, D. C. (2000). Nightmares and bad dreams: their prevalence and relationship to well-being. J. Abnorm. Psychol. 109, 273–281. doi: 10.1037//0021-843x.109.2.273
Zadra, A. L. (1990). “Lucid dreaming, dream control, and the treatment of nightmares,” in Proceedings of the Paper Presented at the Seventh Annual Conference of the Association for the Study of Dreams, (Chicago).
Keywords: lucid dreaming, nightmare, rapid eye movement sleep, post-traumatic stress disorder, depression, anxiety
Citation: Macêdo TCF, Ferreira GH, Almondes KM, Kirov R and Mota-Rolim SA (2019) My Dream, My Rules: Can Lucid Dreaming Treat Nightmares? Front. Psychol. 10:2618. doi: 10.3389/fpsyg.2019.02618
Received: 23 July 2019; Accepted: 06 November 2019;
Published: 26 November 2019.
Edited by:
Megan Peters, University of California, Riverside, United StatesReviewed by:
Tadas Stumbrys, Vilnius University, LithuaniaMichael Schredl, Central Institute of Mental Health, Germany
Copyright © 2019 Macêdo, Ferreira, Almondes, Kirov and Mota-Rolim. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Tainá Carla Freitas de Macêdo, tainacarlafreitasdemacedo@gmail.com; Sérgio Arthuro Mota-Rolim, sergioarthuro@neuro.ufrn.br
†These authors have contributed equally to this work and share last authorship