 Anna Guerrini Usubini1,2
Anna Guerrini Usubini1,2 Giorgia Varallo1,2Valentina Granese1,2
Giorgia Varallo1,2Valentina Granese1,2 Roberto Cattivelli1,2
Roberto Cattivelli1,2 Simone Consoli1Ilaria Bastoni1Clarissa Volpi1
Simone Consoli1Ilaria Bastoni1Clarissa Volpi1 Gianluca Castelnuovo1,2*Enrico Molinari1,2
Gianluca Castelnuovo1,2*Enrico Molinari1,2- 1Istituto Auxologico Italiano, Psychology Research Laboratory, Milan, Italy
- 2Department of Psychology, Catholic University of Milan, Milan, Italy
Obesity is a global health problem that affects both physical and psychological health and well-being. Psychological flexibility is one of the key components related to psychological health. This cross-sectional study aims to investigate the impact of psychological flexibility on psychological well-being in a sample of 220 individuals with obesity. Multivariate analysis was performed to investigate the role of psychological flexibility in explaining psychological well-being, controlling for confounding factors (sex, age, and Body Mass Index). According to the results, psychological flexibility significantly explained psychological well-being. Our study provides additional evidence of the impact of psychological flexibility on psychological well-being. It also provides further support for the importance of integrating psychological flexibility in the psychological interventions for obesity.
Introduction
Obesity is a chronic health condition determined by excessive accumulation of adipose tissue, generally explained through the interaction of two conditions: excessive food intake and inadequate levels of physical activity (Castelnuovo et al., 2017). Obesity is a complex disease with a multifactorial etiology. Genetic, metabolic, as well as socio-cultural, behavioral, and environmental factors contribute to determining a condition of obesity (Curry, 2013; Boles et al., 2017). Also, both sexes and all ages are affected by obesity (World Health Organization Technical Report Series, 2000). Over the last fifty years, obesity has increased considerably, reaching pandemic levels. In 2014, more than 1 billion people worldwide were overweight. Of these, over 600 million meet the criteria for obesity based on Body Mass Index (BMI: Kg/m2 > 30) (World Health Organization Technical Report Series, 2000).
Obesity is considered a risk factor for many medical complications and comorbidities. Specifically, it impairs both physical and psychological well-being. It increases risks for metabolic, cardiovascular, and musculoskeletal diseases, such as type 2 diabetes, hypertension, and osteoarthritis as well as some types of cancer, dyslipidemia hypercholesterolemia and obstructive sleep apnea syndrome. Similarly, obesity and overweight are associated with a broad variety of psychological consequences such as depression, anxiety, eating disorders, lower quality of life, and lower self-esteem (Bray et al., 2017).
Most of the research on psychological flexibility has been conducted within the context of Acceptance and Commitment Therapy (ACT) (Hayes et al., 2006), a transdiagnostic approach raised in the third-wave Cognitive-behavioral Therapies (CBTs). According to ACT, acceptance of unpleasant experiences is more helpful than attempts to directly control inner events. Therefore, the aim of ACT is to promote psychological flexibility, defined as “the ability to directly and openly contact experience in the present moment and persisting or changing behavior according to what the situation affords and one's personal goals and values” (Hayes et al., 2006). Psychological flexibility is considered as a broad, overarching psychological process, resulting from the action of six key components: cognitive defusion (i.e., learning to distance from a person's thoughts); acceptance (i.e., an open attitude to painful inner experiences, including feelings, emotions, and thoughts); being in touch with the present moment; self as a context (i.e., contacting a stable sense of self regardless of one's personal experiences); finally, committed actions (i.e., pursuing actions or stable behaviors driven by personal values).
Numerous empirical studies have examined the efficacy of ACT in a variety of health conditions. Recently, a meta-analysis highlights that ACT was effective in reducing psychological distress and improving quality of life and a sense of hope in individuals with cancer (Zhao et al., 2021). In a randomized controlled trial, an ACT-based group intervention improved the quality of life, physical and psychological well-being in a sample of individuals with myocardial infarction (Ghahnaviyeh et al., 2020). Moreover, psychological flexibility was associated with health benefits in a range of clinical disorders (Powers et al., 2009; Kashdan and Rottenberg, 2010; Cattivelli et al., 2018) including anxiety and depressive symptomatology (Twohig and Levin, 2017) as well as chronic pain (Vowles and McCracken, 2008) and stress (Cristina et al., 2018). Together, these findings suggest that psychological flexibility is a key factor for the quality of life and psychological well-being (Biglan et al., 2008). The impact of ACT on psychological flexibility has been shown to help persons with obesity deal with self-stigma (Lillis et al., 2009), reduce binge eating (Lillis et al., 2011), and as a result of these changes improve quality of life and reduce weight (Lillis et al., 2009, 2011).
The study of psychological flexibility in individuals with obesity is still in its infancy. Few studies have examined this population. However, from previous evidence, it appears to be a promising aspect to be taken into account in the promotion of psychological well-being (Weineland et al., 2012; Cattivelli et al., 2018; Schumacher et al., 2019). It's therefore important to evaluate this aspect in individuals with obesity as well.
For this reason, the aim of the study is to evaluate the association between psychological flexibility and psychological well-being in a sample of individuals with obesity. In this study, we have focused on a definition of psychological well-being which highlights self-perceived health and psychological aspects of well-being, including both positive and negative intrapersonal affective or emotional states, emphasizes the individual, subjective appraisals (Diener, 1984; Dupuy, 1990; Grossi and Compare, 2014).
In the present cross-sectional study, we aimed at (1) evaluating the relationship between psychological flexibility and general psychological well-being in a sample of individuals affected by obesity; secondly, we aimed to (2) assess the role of psychological flexibility in explaining levels of psychological well-being. We hypothesized that (1) psychological flexibility would show a significant correlation with psychological general well-being; and that (2) psychological flexibility would explain significant and unique variance of indices of psychological general well-being.
Materials and Methods
Participants
The participants were 220 Italian obese adults 122 females (55,4%), 98 males (44,5%) aged between 18 and 87, who were consecutively recruited from the Istituto Auxologico Italiano, Ospedale S. Giuseppe, Piancavallo located in Northern Italy, at the beginning of a month-long hospitalization for weight loss. Only individuals with obesity (BMI ≥ 30) are eligible for hospitalization.
In-patients were eligible for the study if they met the following inclusion criteria: (1) age > 18 years; (2) BMI (Kg/m2) > 30; (3) written and informed consent to participate. Patients were excluded from the study if they did not meet the criteria for obesity (BMI ≥ 30) and had: (1) severe psychiatric disturbance diagnosed with the criteria of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5); (2) concurrent severe medical condition that could compromise the participation in the study (e.g., blindness, deafness, neurological disorder, physical disability).
Measures
Demographic data (i.e., sex, age, work status, etc.) were collected using a self-report form. The BMI was determined by the physician who, when the patient was admitted to the hospitalization, carried out the assessment visit.
To evaluate the independent variable, we used the Acceptance and Action Questionnaire (AAQ-II) (Bond et al., 2011). The AAQ-II is composed of 10 items (e. g “I am afraid of my feelings,” “I worry about not being able to control my worries and feelings”) rated from 1–7, on a 7-point Likert scale. It is the most widely used self-reported questionnaire that provides a measure of psychological flexibility. Higher total scores mean less flexibility, while lower total scores mean more flexibility. Scores range from a minimum of 0 to a maximum of 70. We used the Italian Validation (Pennato et al., 2013) that showed good psychometric properties, in agreement with the original version.
To evaluate the outcome, we used the Psychological General Well-Being Inventory (PGWBI) (Dupuy, 1990). The PGWBI is a validated measure widely used in clinical practice and research to provide a general subjective assessment of psychological well-being and health. We used the Italian validation of Grossi and colleagues (Grossi and Compare, 2014) that showed good psychometric properties in agreement with the original version. The questionnaire consists of 22 self-administered items rated on 6 point Likert scale ranged from 0 to 5 exploring six dimensions: anxiety (PGWBI_A; e.g., “Have you been bothered by nervousness or your “nerves” during the past month?”), depressed mood (PGWBI_D; e.g., “I felt downhearted and blue during the past month”), positive well-being (PGWBI_PWB; e.g., “I felt cheerful, lighthearted during the past month.”), self-control (PGWBI_SC; e.g., “I was emotionally stable and sure of myself during the past month”), general health (PGWBI_GH; e.g., “How have you been feeling in general during the past month?”), and vitality (PGWBI_V; e.g., “I felt tired, worn out, used up, or exhausted during the past month”). The six subscales consist of a minimum of three to a maximum of five items. The scores of all domains can be summarized to provide a summary score, which ranges from a minimum of 0 to a maximum of 110 points, representing the best achievable well-being.
Procedures
At the beginning of the hospitalization, all patients underwent a clinical interview conducted by a clinical psychologist, to assess for current or pre-existing diagnosis of psychiatric disturbances. Patients diagnosed with psychiatric disorders were not selected for the study. According to eligibility criteria all recruited patients were asked to fill out the questionnaires abovementioned at the time of admission to the rehabilitation program. After providing informed and written consent to participate, questionnaires were administered in a research room, under the supervision of a psychologist involved in the research team. Data were collected from 1st December 2019 to 3rd March 2020.
The Medical Ethics Committee approved the study protocol and Informed Consent. All participants read, understood, and signed an informed consent document. All procedures on human subjects were conducted following the Helsinki Declaration of 1975, as revised in 1983.
Statistical Analysis
The a-priori sample size was estimated for a Linear multiple regression: Fixed model, R2 deviation from zero using G.Power (version 3.1.9.4) (Faul et al., 2007) setting a small effect size (f2 = 0.10), an alpha of.05 and a power of.95, resulting in 191 participants.
Descriptive statistics have been conducted to describe the sample, detect missing values, and assess the normality of distributions. Descriptive statistics were calculated in terms of means and standard deviation for continuous variables, and in terms of frequencies and percentage for categorical variables.
Pearson's bivariate correlations have been computed to investigate the association between psychological flexibility and psychological well-being. A hierarchical regression analysis was then conducted to evaluate the contribution of the AAQ-II total score to the variance of the PGWBI total score. AAQ-II was set as the independent variable, controlling for sex, age and, BMI as possible confounding variables, and the total score of PGWBI was set as dependent variable. Confounding factors, that are likely to affect the main outcome were included in the first block; the AAQ-II total score was included in the second block. ΔR2 was used to evaluate the additional amount of variance in the dependent variable, which was accounted for by the AAQ-II score included in the second block compared to the first block including only confounding factors. Then, a MANOVA was performed to help protect against inflating the Type 1 error rate (Richard and Wichern, 2002). We set age, sex, BMI, and AAQ-II score as independent variables, and all subscales of the PGWBI as dependent variables.
Missing data lower than 5% was considered inconsequential (Schafer and Olsen, 1998). P-values <0.05 were considered statistically significant. Partial η-square values were interpreted according to Cohen (small = 0.01; medium = 0.06; large = 0.14; Cohen, 1977). The analyses were performed using Statistical Package for the Social Sciences (SPSS) version 26.
Results
Participants Characteristics
The sample was composed by 122 (55,5%) females and 98 males (44,5%) aged (in years) between 18 and 87 (M = 55.61; SD = 12.58), the average BMI (Kg/m2) was 43.66 ± 7.76. Almost half of the participants were married (48.9%) and had a high school degree (48.2%) and were employed (36.5%). Descriptive statistics of the sample were presented in Table 1.
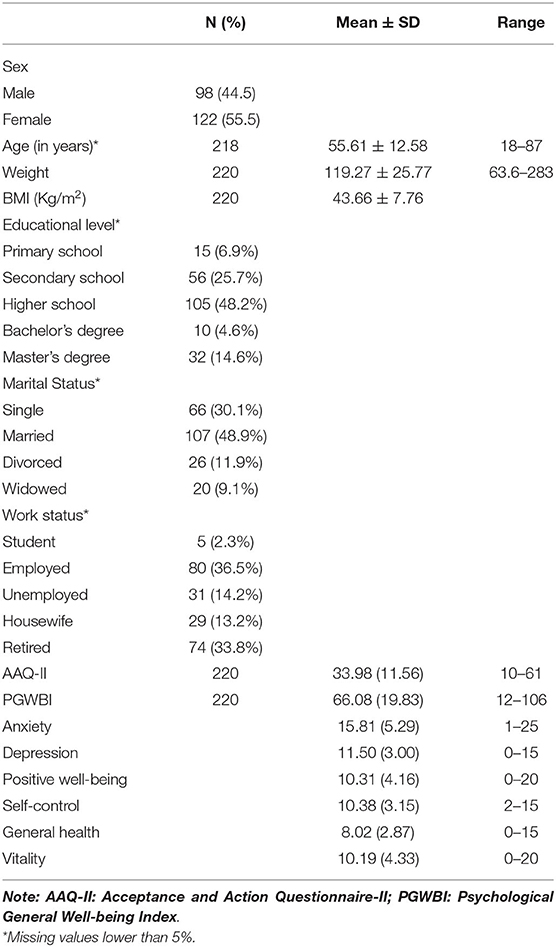
Table 1. Descriptive statistics of the sample.
Correlations
To assess the association between psychological flexibility and psychological well-being, correlational analyses were performed. AAQ-II resulted significantly and negatively related to all the PGWBI subscales. Correlations are presented in Table 2.
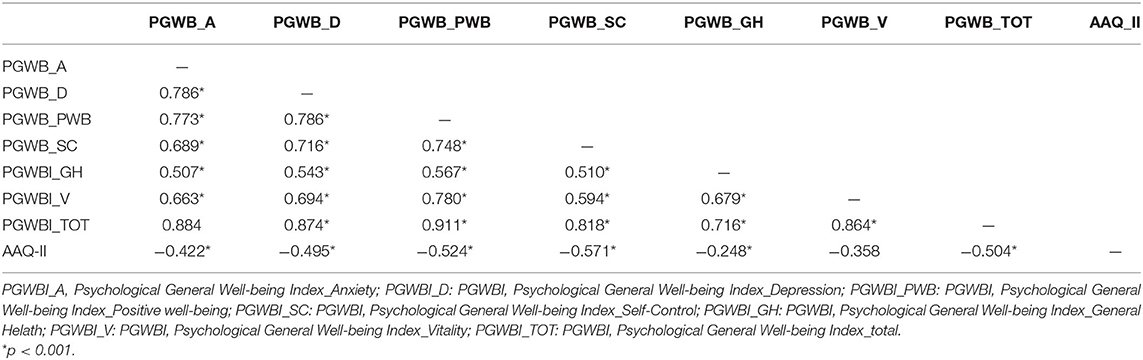
Table 2. Correlations.
Psychological General Well-Being
The full model of age, sex, BMI, AAQ-II score as the independent variables and PGWBI total score as the dependent variable was statistically significant, R2 = 0.265, Adjusted R2 = 0.270, [F(4, 202) = 20.06]; p < 0.001. The inclusion of the AAQ-II score, compared to the first block including only the confounding factors, explained about 24% additional variance, ΔR2 = 0.240; [F(1, 202) = 67.8]; p < 0.001. Only the AAQ-II score significantly explained the PGWBI total score (Table 3).
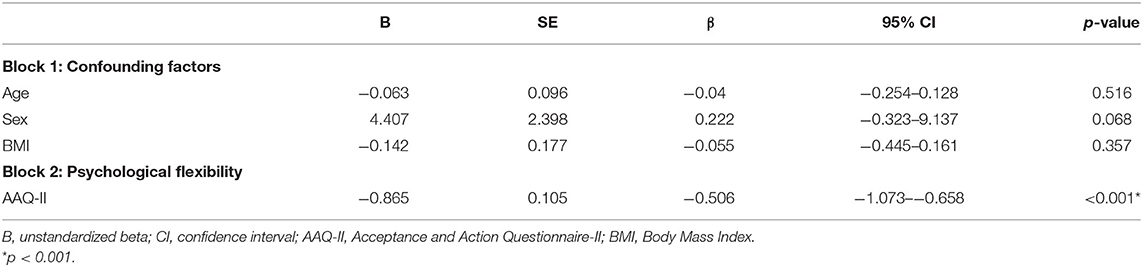
Table 3. Multivariable linear regression model examining the independent effect of demographic features and psychological flexibility (AAQ-II total score) on psychological well-being (PGWBI total score).
Multivariate Analysis
We also conducted multivariate analysis to assess the role of psychological flexibility in explaining all the subscales of PGWBI, controlling for sex, age and BMI (Table 4). Gender served as fixed factor, while age, BMI and AAQ-II served as covariates. All the subscale of PGWBI were included as dependent variables. Only, the AAQ-II has a statistically significant effect on all PGWBI subscales, [F(6, 197) = 18.723]; p < 0.001; partial η2 = 0.363. Both sex [F(6, 197) = 1.634; p = 0.140; partial η2 = 0.047], and age [F(6, 197) = 2.051; p = 0.61; partial η2 = 0.59] and BMI [F(6, 197) = 1.382; p = 0.224; partial η2 = 0.040] resulted statistically non-significant.
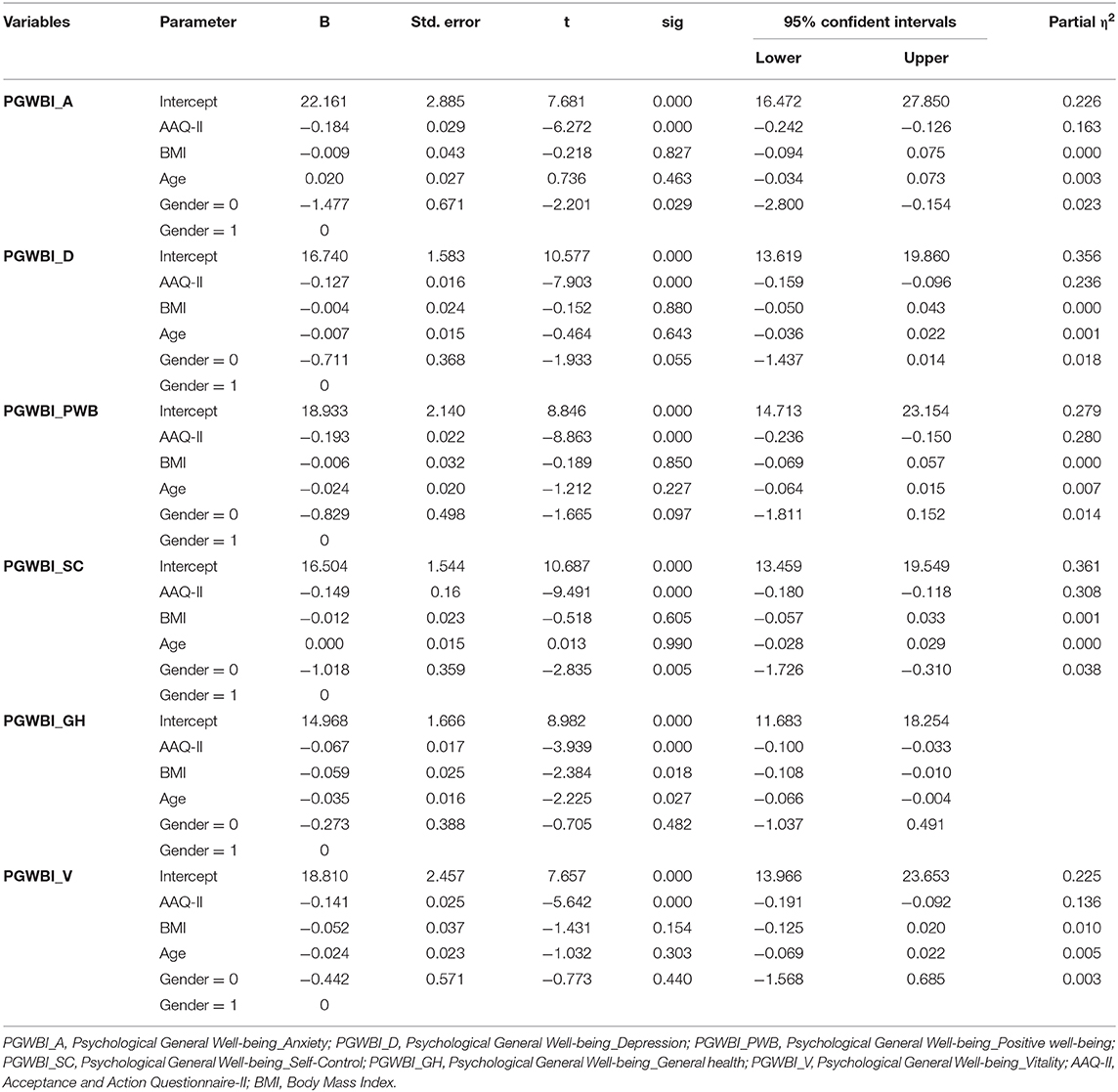
Table 4. Parameter estimates.
As reported in the parameter estimates table below, AAQ-II significantly explained all subscales of the PGWBI. Sex was statistically significant in the Anxiety and Self-control subscales. The BMI and Age were statistically significant only in the General Health subscale. Parameter estimates have been reported in Table 4.
Discussion
With respect to our first hypothesis, the results of the present study showed a statistically significant association between psychological flexibility and psychological well-being and health. The AAQ-II score resulted negatively and significantly correlated with psychological general well-being and all its separate dimensions (anxiety, depressive mood, positive well-being, general health, self-control, and vitality) in individuals with obesity. This means that less psychological flexibility is related to lower levels of psychological well-being.
With respect to our second hypothesis, according to the results psychological flexibility explained a statistically significant proportion of psychological well-being and its dimensions, when controlling for demographical and clinical factors, with proven explanatory value (Eichstaedt et al., 2020).
Our findings are consistent with the evidence supporting the psychological flexibility model developed by Hayes et al. (2006) in the field of ACT. According to this model, people who have higher levels of psychological well-being can establish an open and flexible contact with their own internal and external states (environmental) and engage themselves in committed actions related to personal values. Psychological flexibility has been strongly associated with several positive psychological outcomes, such as increased psychological well-being, reduced stress, anxiety, and depressive symptomatology (Bardeen et al., 2014; Francis et al., 2016; Tyndall et al., 2020). In opposition, decreased levels of psychological flexibility form the basis of psychological distress characterized by difficulties in emotional and behavioral regulation (Masuda and Tully, 2012).
Nowadays, current guidelines for obesity management strongly recommend providing comprehensive multi-professional and multidisciplinary interventions including exercise, diet, and behavioral or cognitive-behavioral therapy to promote healthy lifestyle change and psychological well-being. The current study has important clinical implications. Given the pandemic diffusion of obesity and in light of the well-documented poorer psychological health of individuals with obesity (Finger et al., 2020), it's important to address psychological factors related to obesity. To do so, identifying modifiable dimensions that influence psychological well-being, as psychological flexibility, should be the preliminary step to provide effective interventions.
Our study provides additional support to the existence of a link between psychological flexibility and well-being. This could be a valid promising result supporting the application of ACT-based intervention for individuals with obesity. Further studies are required to address the validity of such interventions, but some evidence has been already collected (Forman et al., 2013, 2016, 2019; Cattivelli et al., 2018).
Several limitations of the study must be addressed. First, all the data were cross-sectional, which warrants caution in drawing causal conclusions, although our goal was not to investigate causality. Secondly, the sample was composed exclusively of hospitalized individuals, which may induce a selection bias: thus, generalization to patients from different settings should be carefully done. Besides, our sample was composed of patients with a wide range of ages. Also, we did not investigate the presence of eating disorders in our sample. This may limit the generalizability of the results achieved.
On the other hand, this article has several strengths, which include the use of validated, reliable survey instruments, as well as an adequate sample size, and the fact that it presents data on a population on which there is still little research.
Longitudinal studies should be conducted to assess whether the improvement of psychological flexibility could have an effective impact on the psychological status of individuals with obesity and the rehabilitation outcomes, such as the adoption of long-standing healthy lifestyle habits. Future studies should also include individuals with obesity and comorbid eating disorders that were not considered in the present study.
Conclusion
Achieving psychological well-being is one of the most relevant purposes psychological interventions aim for. Identifying the psychological processes that can help to protect psychological well-being is relevant. Findings from the current study suggest that psychological flexibility may be a helpful tool to identify those individuals most at risk of developing poor psychological well-being. Moreover, they provide additional evidence of the beneficial role of psychological flexibility on well-being and provides further support for the utility of enhancing psychological flexibility in the psychological interventions for obesity.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by Istituto Auxologico Italiano. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
AG and GV conceived the study, planned the design, made a substantial contribution to the manuscript drafting, defined the statistical analysis, and establish the sample size for the study. VG, RC, SC, IB, and CV contributed greatly to the manuscript drafting. GC and EM read and approved the final manuscript. All authors contributed to the article and approved the submitted version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
Bardeen, J., Fergus, T., and Orcutt, H. (2014). Experiential avoidance as a moderator of the relationship between anxiety sensitivity and perceived stress. Behav. Ther. 44, 459–469. doi: 10.1016/j.beth.2013.04.001
Biglan, A., Hayes, S. C., and Pistorello, J. (2008). Acceptance and commitment: implications for prevention science. Prev. Sci. 9, 139–152. doi: 10.1007/s11121-008-0099-4
Boles, A., Kandimalla, R., and Reddy, P. H. (2017). Dynamics of diabetes and obesity: epidemiological perspective. Biochim. Biophys. Acta Mol. Basis Dis. 1863, 1026–1036. doi: 10.1016/j.bbadis.2017.01.016
Bond, F. W., Hayes, S. C., Baer, R. A., Carpenter, K. M., Guenole, N., Orcutt, H. K., et al. (2011). Preliminary psychometric properties of the acceptance and action questionnaire-II: a revised measure of psychological inflexibility and experiential avoidance. Behav. Ther. 42, 676–688. doi: 10.1016/j.beth.2011.03.007
Bray, G. A., Kim, K. K., and Wilding, J. P. H. (2017). Obesity: a chronic relapsing progressive disease process. A position statement of the World Obesity Federation. Obes. Rev. 18, 715–723. doi: 10.1111/obr.12551
Castelnuovo, G., Pietrabissa, G., Manzoni, G. M., Cattivelli, R., Rossi, A., Novelli, M., et al. (2017). Cognitive behavioral therapy to aid weight loss in obese patients: current perspectives. Psychol. Res. Behav. Manag. 10, 165–173. doi: 10.2147/PRBM.S113278
Cattivelli, R., Castelnuovo, G., Musetti, A., Varallo, G., Spatola, C. A. M., Riboni, F. V., et al. (2018). ACTonHEALTH study protocol: promoting psychological flexibility with activity tracker and mHealth tools to foster healthful lifestyle for obesity and other chronic health conditions. Trials 19, 1–11. doi: 10.1186/s13063-018-2968-x
Cristina, P. M., Marinella, C., Tiziana, M., Minissale, C., Concetta, D. P., D'orto, et al. (2018). Successfully aging. Choice of life or life that choices? Acta Med. Mediterr. 34, 107–111. doi: 10.19193/0393-6384
Diener, E. (1984). Subjective well-being. Psychol. Bull. 95, 542–575. doi: 10.1037/0033-2909.95.3.542
Dupuy, H. J. (1990). “The Psychological General Well-Being (PGWB) index,” in Assessment of Quality of Life in Clinical Trials of Cardiovascular Therapies, eds J. E. K. Wenger, M. E. Mattson, and C. D. Furburg (Le Jacq Publishing), 170–183.
Eichstaedt, J. C., Yaden, D. B., Ribeiro, F. M., Adler, A., and Kern, M. L. (2020). Lifestyle and wellbeing: exploring behavioral and demographic covariates in a large us sample. Int. J. Wellbeing 10, 87–112. doi: 10.5502/ijw.v10i4.831
Faul, F., Erdfelder, E., Lang, A. G., and Buchner, A. (2007). G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 39, 175–191. doi: 10.3758/BF03193146
Finger, I., de Freitas, B. I., and Oliveira, M. (2020). Psychological inflexibility in overweight and obese people from the perspective of acceptance and commitment therapy (ACT). Eat. Weight Disord. 25, 169–175. doi: 10.1007/s40519-018-0541-y
Forman, E. M., Butryn, M. L., Juarascio, A. S., Bradley, L. E., Lowe, M. R., Herbert, J. D., et al. (2013). The mind your health project: a randomized controlled trial of an innovative behavioral treatment for obesity. Obesity 21, 1119–1126. doi: 10.1002/oby.20169
Forman, E. M., Butryn, M. L., Manasse, S. M., Crosby, R. D., Goldstein, S. P., Wyckoff, E. P., et al. (2016). Acceptance-based versus standard behavioral treatment for obesity: results from the mind your health randomized controlled trial. Obesity 24, 2050–2056. doi: 10.1002/oby.21601
Forman, E. M., Manasse, S. M., Butryn, M. L., Crosby, R. D., Dallal, D. H., and Crochiere, R. J. (2019). Long-term follow-up of the mind your health project: acceptance-based versus standard behavioral treatment for obesity. Obesity 27, 565–571. doi: 10.1002/oby.22412
Francis, A. W., Dawson, D. L., and Golijani-Moghaddam, N. (2016). The development and validation of the Comprehensive assessment of Acceptance and Commitment Therapy processes (CompACT). J. Context. Behav. Sci. 5, 134–145. doi: 10.1016/j.jcbs.2016.05.003
Ghahnaviyeh, L. A., Bagherian, R., Feizi, A., Afshari, A., and Darani, F. M. (2020). The effectiveness of acceptance and commitment therapy on quality of life in a patient with myocardial infarction: a randomized control trial. Iran. J. Psychiatry 15, 1–9. doi: 10.18502/ijps.v15i1.2434
Grossi, E., and Compare, A. (2014). “Psychological General Well-Being Index (PGWB),” in Encyclopedia of Quality of Life and Well-Being Research, 5152–5156. doi: 10.1007/978-94-007-0753-5_2309
Hayes, S. C., Luoma, J. B., Bond, F. W., Masuda, A., and Lillis, J. (2006). Acceptance and commitment therapy: model, processes and outcomes. Behav. Res. Ther. 44, 1–25. doi: 10.1016/j.brat.2005.06.006
Kashdan, T. B., and Rottenberg, J. (2010). Psychological flexibility as a fundamental aspect of health. Clin. Psychol. Rev. 30, 865–878. doi: 10.1016/j.cpr.2010.03.001
Lillis, J., Hayes, S. C., Bunting, K., and Masuda, A. (2009). Teaching acceptance and mindfulness to improve the lives of the obese: a preliminary test of a theoretical model. Ann. Behav. Med. 37, 58–69. doi: 10.1007/s12160-009-9083-x
Lillis, J., Levin, M. E., and Hayes, S. C. (2011). Exploring the relationship between body mass index and health-related quality of life: a pilot study of the impact of weight self-stigma and experiential avoidance. J. Health Psychol. 16, 722–727. doi: 10.1177/1359105310388321
Masuda, A., and Tully, E. C. (2012). The role of mindfulness and psychological flexibility in somatization, depression, anxiety, and general psychological distress in a nonclinical college sample. J. Evid. Based Complement. Alternat. Med. 17, 66–71. doi: 10.1177/2156587211423400
Pennato, T., Berrocal, C., Bernini, O., and Rivas, T. (2013). Italian version of the acceptance and action questionnaire-II (AAQ-II): dimensionality, reliability, convergent, and criterion validity. J. Psychopathol. Behav. Assess. 35, 552–563. doi: 10.1007/s10862-013-9355-4
Powers, M. B., Zum, M. B., Sive, V., and Paul, V. (2009). Acceptance and commitment therapy: a meta-analytic review. Psychoter. Psychosom. 78, 73–80. doi: 10.1159/000190790
Richard, A. J., and Wichern, D. W. (2002). Applied Multivariate Statistical Analysis. London: Prenticee Hall.
Schafer, J. L., and Olsen, M. K. (1998). Multiple imputation for multivariate missing-data problems: a data analyst's perspective. Multivar. Behav. Res. 33, 545–571.
Schumacher, L. M., Godfrey, K. M., Forman, E. M., and Butryn, M. L. (2019). Change in domain-specific but not general psychological flexibility relates to greater weight loss in acceptance-based behavioral treatment for obesity. J. Context. Behav. Sci. 12, 59–65. doi: 10.1016/j.jcbs.2019.01.008
Twohig, M. P., and Levin, M. E. (2017). Acceptance and commitment therapy as a treatment for anxiety and depression: a review. Psychiatr. Clin. North Am. 40, 751–770. doi: 10.1016/j.psc.2017.08.009
Tyndall, I., Waldeck, D., Pancani, L., Whelan, R., Roche, B., and Pereira, A. (2020). Profiles of psychological flexibility: a latent class analysis of the acceptance and commitment therapy model. Behav. Modif. 44, 365–393. doi: 10.1177/0145445518820036
Vowles, K. E., and McCracken, L. M. (2008). Acceptance and values-based action in chronic pain: a study of treatment effectiveness and process. J. Consult. Clin. Psychol. 76, 397–407. doi: 10.1037/0022-006X.76.3.397
Weineland, S., Hayes, S. C., and Dahl, J. (2012). Psychological flexibility and the gains of acceptance-based treatment for post-bariatric surgery: six-month follow-up and a test of the underlying model. Clin. Obes. 2, 15–24. doi: 10.1111/j.1758-8111.2012.00041.x
World Health Organization Technical Report Series (2000). Obesity: Preventing and Managing the Global Epidemic. Report of a WHO consultation on obesity. Geneva: World Health Organization.
Zhao, C., Lai, L., Zhang, L., Cai, Z., Ren, Z., Shi, C., et al. (2021). The effects of acceptance and commitment therapy on the psychological and physical outcomes among cancer patients: a meta-analysis with trial sequential analysis. J. Psychosom. Res. 140:110304. doi: 10.1016/j.jpsychores.2020.110304
Keywords: psychological flexibility, psychological well-being, health psychology, Acceptance and Commitment Therapy, obesity, rehabilitation
Citation: Guerrini Usubini A, Varallo G, Granese V, Cattivelli R, Consoli S, Bastoni I, Volpi C, Castelnuovo G and Molinari E (2021) The Impact of Psychological Flexibility on Psychological Well-Being in Adults With Obesity. Front. Psychol. 12:636933. doi: 10.3389/fpsyg.2021.636933
Received: 02 December 2020; Accepted: 22 February 2021;
Published: 22 March 2021.
Edited by:
Diogo Lamela, Universidade Lusófona, PortugalReviewed by:
Eva M. Conceição, University of Minho, PortugalGiovambattista Presti, Kore University of Enna, Italy
Copyright © 2021 Guerrini Usubini, Varallo, Granese, Cattivelli, Consoli, Bastoni, Volpi, Castelnuovo and Molinari. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Gianluca Castelnuovo, gianluca.castelnuovo@auxologico.it