 María A. Olivencia-Carrión
María A. Olivencia-Carrión Isabel Ramírez-Uclés
Isabel Ramírez-Uclés Pablo Holgado-Tello
Pablo Holgado-Tello Francisca López-Torrecillas1*
Francisca López-Torrecillas1*- 1Center for Research into the Mind, Brain and Behavior, Granada University, Granada, Spain
- 2Department of Personality, Assessment and Psychological Treatment, Universidad Nacional de Educación a Distancia, Madrid, Spain
- 3Department of Behavioral Sciences Methodology, Universidad Nacional de Educación a Distancia, Madrid, Spain
Mobile phone addiction has attracted much attention recently and is showing similarity to other substance use disorders. Because no studies on mobile phone addiction had yet been conducted in Spain, we developed and validated a questionnaire (Cuestionario de Abuso del Teléfono Móvil, ATeMo) to measure mobile phone abuse among young adults in Spanish. The ATeMo questionnaire was designed based on relevant DSM-5 diagnostic criteria and included craving as a diagnostic symptom. Using stratified sampling, the ATeMo questionnaire was administered to 856 students (mean age 21, 62% women). The MULTICAGE questionnaire was administered to assess history of drug abuse and addiction. Using confirmatory factor analysis, we found evidence for the construct validity of the following factors: Craving, Loss of Control, Negative Life Consequences, and Withdrawal Syndrome, and their association with a second order factor related to mobile phone abuse. The four ATeMO factors were also associated with alcoholism, internet use, and compulsive buying. Important gender differences were found that should be considered when studying mobile phone addictions. The ATeMo is a valid and reliable instrument that can be used in further research on mobile phone abuse.
Introduction
The mobile phone has many characteristics that make it attractive to young adults. It is primarily used to communicate but also has many other interesting applications, including camera, internet, music reproduction, games, and social media. The International Telecommunication Union report (The International Telecommunication Union, 2016) finds that 98% of young adults own a mobile phone in Europe and other studies indicate that young women in particular have more interest in mobile phones than other groups do (Roberts et al., 2014). There is evidence that mobile phone abuse in related to physical and mental wellbeing problems, including social and psychological disturbances such as attention deficit and hyperactivity disorder, disruptive behavior disorders, anxiety disorders, mood disorders, substance use disorders, sleep disorders, and eating disorders (Billieux et al., 2014; Foerster et al., 2015). In recent years, a co-occurrence has been established between mobile phone dependence and other behavioral disorders such as internet addiction (Chiu et al., 2013), compulsive buying (Jiang and Shi, 2016) and alcohol use (De-Sola et al., 2017a) or use of other substances (Gallimberti et al., 2016). However, it remains unclear if an individual that develops one addictive behavior (i.e., mobile phone abuse) is more likely to develop another addictive behavior or a substance use problem.
Although a definition of mobile phone abuse has not yet been agreed upon, some researchers define mobile phone dependence as a constant use of the device with a poor capacity to control daily activities, exhibiting extreme nervousness and aggressive behavior when deprived of its use; this excessive use is also accompanied by a progressive deterioration in school/work performance and social and family functioning (Billieux et al., 2014; Lin et al., 2015). These symptoms have a major negative impact on the life of the affected person, reflected in impaired health or deprived social functioning; they have also been shown to be equivalent to substance dependence as understood by the current nosological systems Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5, American Psychiatric Association, 2012).
Mobile phone addiction could in many ways be similar to substance dependence disorders (Foerster et al., 2015; Roser et al., 2016). For instance, the abuse of psychotropic drugs (heroin, cocaine, cannabis, etc.) and alcohol is a complex social, biological, and psychological phenomenon. Whether an individual ever uses alcohol or another substance, and whether that initial use progresses to a substance use disorder of any severity, depends on a number of factors. These include: a person's genetic makeup and other individual biological factors; psychological factors related to a person's unique history and personality; and environmental factors, such as the availability of drugs, family and peer dynamics, coping with stress, and access to social support. Chronic consumption of several drugs (cannabis, stimulants, and opioids) has been associated with the presence of neuropsychological impairments in a broad range of functions. In recent years neuropsychological research on substance abuse has focused on the study of impairments in executive functions linked to the prefrontal cortex and their influence on the personality, cognitions, and behaviors of the substance abusers (López-Torrecillas et al., 2000; Verdejo-García et al., 2004).
To date, pathological gambling is the non-substance related addiction which has received most attention and has been examined extensively. The results reveal a number of substantial similarities between pathological gambling and substance-related addictions concerning phenomenology, epidemiology, personality factors, genetics, neurobiological processes, recovery, and treatment (Walther et al., 2012; Contreras-Rodríguez et al., 2016; Navas et al., 2017). In DSM-5, pathological gambling is classified as a non-substance-related addiction and is, therefore, removed from the former category “Impulse-Control Disorders” and included in the new “Substance Use and Addictive Disorders” category. Other potential non-substance-related addictions are internet addiction, compulsive buying, sex addiction, and mobile phone addiction, although these are not yet officially defined as disorders due to a lack of evidence. Despite a substantial overlap, it is not yet clear why some people become vulnerable to these behaviors. The co-occurrence of non-substance-related addiction with different forms of substance abuse such as smoking, drinking, use of cannabis, and other illegal drugs among young people has been repeatedly discussed (Vanyukov et al., 2012; De-Sola et al., 2017a).
The literature also reveals an association between multiple substance use and other risk behaviors among young adults. For example, binge drinking, cannabis use, and tobacco use appear to be more prevalent in young people (Van Rooij et al., 2014; Abebe et al., 2015). The use of both alcohol and cannabis predicts use of common addictive substances (Osuch et al., 2013; Viola et al., 2014; Vorspan et al., 2015) and tends to be accompanied by gambling (Larsen et al., 2013; Míguez and Becoña, 2015). In addition, a number of authors (Mudry et al., 2011; Yau et al., 2012; Grant et al., 2013; Lee et al., 2013; Mattebo et al., 2013; Schuster et al., 2013; Van Rooij et al., 2014; Biolcati, 2015) have pointed out the relationship between the amount of time young adults spend gambling, abusing their mobile phones, using the internet, playing video games, buying compulsively, or having sex and increases in alcohol, tobacco, cannabis, and drug consumption.
The acknowledgement of behavioral addictions as disorders can be traced as far back as Marlatt et al. (1988), who reported a repetitive habit pattern that increases the risk of disease and/or associated personal and social problems. Addictive behaviors are often experienced subjectively as a loss of control in which the behavior continues to occur despite volitional attempts to abstain or moderate use. Furthermore, in the last decade, a growing number of studies have established psychological and neurobiological similarities between the excessive practice of addictive behaviors (e.g., mobile phone abuse, compulsive buying, sex, internet, video gaming, and eating disorders; Billieux et al., 2010; Mentzoni et al., 2011). Research on the neurobiology of addiction has also found a common mechanism between substance addictions and behavioral addictions (Leeman and Potenza, 2013; Weinstein and Lejoyeux, 2015). However, at this point we do not know whether having one addictive behavior increases the likelihood of developing other addictive behaviors or other dependencies such as substance use disorders. In addition, alcohol, drugs, and pathological gambling may not be the only crippling addictions that we should address. Unfortunately, other addiction statistics are scarce because many destructive habits are not yet officially recognized as addictions, including mobile phone addiction, game addiction, eating, shopping, and sex addiction, all of which are problematic for many reasons. They all involve direct manipulation of pleasure through the use of products, similar to drug use disorders and food-related disorders.
The concept of non-substance-related (or “behavioral”) addiction describes syndromes analogous to substance addiction, but with a focus on a certain behavior which, similar to substance consumption, produces short-term reward and may persist despite harmful consequences due to diminished control over the behavior. Given that addictive behavior is not necessarily restricted to substance consumption, the DSM-5 broadens the category “Substance-Related Disorders” to a “Substance Use and Addictive Disorders” category including both substance and non-substance-related addictions. The Diagnostic and Statistical Manual of Mental Disorders—4th Edition (DSM-IV; American Psychiatric Association, 2002) conceptualized two discrete substance use disorders (SUD), abuse and dependence, defined by mutually exclusive sets of diagnostic criteria. Abuse required endorsement of one or more (1+) of four abuse criteria, and dependence required endorsement of three or more (3+) of seven dependence criteria. In contrast, the proposed Diagnostic and Statistical Manual of Mental Disorders—5th Edition (DSM-5; American Psychiatric Association, 2012) conceptualizes a unitary SUD construct, varying only in terms of severity. The literature reviewed here includes studies on postulated behavioral addictions related to the use of mobile phones, shopping, sex, internet, video gaming, and food, along with other studies that analyzed the co-occurrence of these addictions with substance abuse (for instance tobacco, alcohol, and cannabis substances). However, these are not included in the DSM-5 because of current lack of evidence. In order to be able to obtain relevant evidence in the first place, we need valid and reliable instruments that allow us to measure addictive behaviors such as mobile phone abuse.
The study of mobile phone abuse started in 2004 with the development of the Mobile Phone Dependency Questionnaire (CPDQ; Toda et al., 2004) designed for use in university populations and validated in a population of high school students by Kawasaki et al. (2006). Another instrument available for use in adult populations is the Mobile Phone Problem Use Scale (MPPUS; Bianchi and Phillips, 2005); including a recent short version (Foerster et al., 2015) and a version for teenagers [Mobile Phone Addiction Scale (MPAS; Leung, 2008)]. This scale has been translated into Japanese (Takao et al., 2009) and Spanish (López-Fernández et al., 2012), with some items previously translated for use in the Spanish university population (Ruiz-Olivares et al., 2010). Although the Mobile Phone Problem Use Scale is one of the most frequently used instruments to assess mobile phone addiction, other instruments exist including the Mobile Phone Usability Questionnaire (MPUQ; Ryu and Smith-Jackson, 2006) and Problematic Mobile Phone Use Questionnaire (PMPUQ; Billieux et al., 2008). In Eastern countries, three scales have been developed: the Mobile Phone Dependence Inventory (MPDI; Xu et al., 2008); the Excessive Cellular Phone Use Survey (ECPUS; Ha et al., 2008), and the Smartphone Addiction Scale (SAS-SV; Kwon et al., 2013). At present there are 5 instruments translated into Spanish: the first one, already mentioned previously—MPPUS, Bianchi and Phillips (2005)—has been adapted by López-Fernández et al. (2012); the second one is the Cell-phone Over-use Scale (COS; Jenaro et al., 2007) for university populations; the third one is the Questionnaire of Mobile-Related Experiences (CERM; Fargues et al., 2009) for adult populations; the fourth one is the Test for Mobile Phone Dependence [TMD] (Chóliz, 2012) for adolescents (including a new reduced version, Chóliz et al., 2016), and finally, the fifth is a questionnaire that focuses only on the dimension of Craving (De-Sola et al., 2017b).
However, no studies have been conducted in Spain to identify mobile phone addiction in young adults using the DSM-5 criteria (American Psychiatric Association, 2012). To this end, it is necessary to develop a valid and reliable instrument measuring mobile addiction, having in mind the modifications made in the DSM-5 (American Psychiatric Association, 2012). These modifications imply that mobile phone addiction should be considered in relation to substance use disorders and behavioral addictions.The diagnostic symptoms of substance use disorders since recently include a new criterion, craving, featured in the DSM-5 (American Psychiatric Association, 2012). One of the most accepted definitions of craving is that of compulsive craving—an irrational and intense desire or uncontrollable compulsion to consume a particular psychoactive substance and/or perform a certain behavior, which leads to compulsive search rituals (Blasco et al., 2008; Igarashi et al., 2008; De-Sola et al., 2017b). Hence, craving should be considered as a criterion to establish a diagnosis and understand the different mediating variables when developing treatments, analyzing relapses, and designing prevention strategies. Therefore, the main purpose of this study was to develop and validate a questionnaire to measure mobile phone dependence among young Spanish speaking adults.
Methods
Participants
The sample comprised of community-dwelling young adults between 17 and 45 years of age (mean 21.12 years old, standard deviation = 3.05, 62.38% women and 37.62% men). They were recruited from the student population of the University of Granada. Participants were recruited by university faculty during class breaks and were selected using a probabilistic sampling design. In particular, a cluster stratified sample design was adopted. Strata were based on the different university faculties. Cluster samples were extracted such that majors and years of study were represented in proportion to the total number of students in each faculty. Finally, all students of the cluster sample were included in the final sample. There were 856 participants recruited between September 2013 and June 2014. The participants were informed about the aims of the study and provided signed informed consent prior to participation. Inclusion criteria were having a mobile phone, wanting to participate, and signing the informed consent form. Prior to recruitment the study was approved by the Research Ethics Committee from the University of Granada, Spain.
Measures
The Mobile Phone Abuse Questionnaire (ATeMo)
The Mobile Phone Abuse Questionnaire (ATeMo) was developed to assess mobile phone dependence. It consists of 25 items covering addictive symptoms, based on the diagnostic criteria for behavioral addiction (gambling) and the DSM-5 (American Psychiatric Association, 2012), and also taking into account substance abuse disorders, and instruments that measure addiction to mobile phones, internet, and social networks. The addictive symptoms considered were craving, loss of control, negative life consequences, and withdrawal syndrome. Specifically, the questionnaire assessed the use of the mobile phone, the disturbance of daily activities, the increase in time spent to obtain the same satisfaction, loss of control, difficulties in stopping using the phone and the irritability produced, and the negative feelings experienced when the mobile phone cannot be used. The 25 items were answered on a 5-point Likert scale that ranged from 0 (strongly disagree) to 4 (strongly agree), resulting in a final score between 0 and 100 (see Table 1).
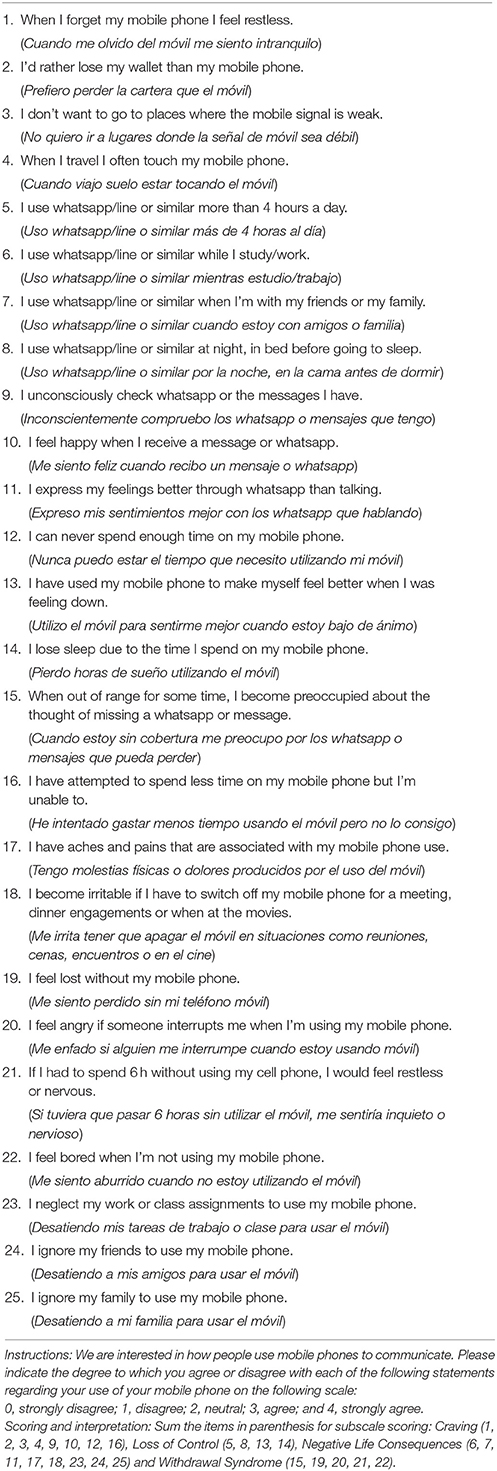
Table 1. Mobile Phone Abuse Questionnaire (ATeMo).
The MULTICAGE CAD-4
The MULTICAGE CAD-4 was designed to screen for a history of drug abuse and addiction behavior. It assesses alcoholism (items 1–4), gambling disorders (items 5–8), drug addiction (items 9–12), eating disorders (items 13–16), internet addiction (items 17–20), video gaming addiction (items 21–24), compulsive buying disorder (items 25–28) and sex addiction (items 29–32). The psychometric properties have been well established in Spanish adult populations. It demonstrates high > 0.7 Cronbach's alpha coefficient. In the exploratory factor analysis, 8 components are identified that identify the proposed structure the diagnostic sensitivity for alcohol was 92.4%, and between 94 and 100% for heroin, cocaine and cannabis (Pedrero-Pérez et al., 2007).
Procedure
The study consisted of two stages: in the first stage the instrument was developed and in the second stage it was validated. The construction of the Mobile Phone Abuse Questionnaire (ATeMo) was based on the DSM-5 (American Psychiatric Association, 2012) that does not recognize mobile addiction as a disorder but makes reference to tobacco addiction and gambling. Ideas were taken from instruments that measure addictions to mobile phones, internet, and social networks and items were created taking into account all the aforementioned. For the construction of the items, criteria for constructing items for Likert questionnaires were used (Jenaro et al., 2007; Billieux et al., 2008; Fargues et al., 2009; Chóliz, 2012; Chóliz et al., 2016; De-Sola et al., 2017a). This set of defined criteria together with the items that evaluated them were reviewed by three experts on clinical psychology, educational psychology, and psychometrics. The experts collaborated in writing and ensuring the understanding, clarity, and consistency in the definitions of the criteria and the items. For the evaluation of the items a5-point rating system was applied (from 0 to 4) taking into account the frequency from never to always (Fishman and Galguera, 2003; Schepers, 2009; Furr, 2011; DeVellis, 2012). Once the expert evaluation was concluded, a pilot experiment was carried out on a sample of 65 university students. They were asked to indicate whether the items in the questionnaire were comprehensible or not, encouraging them to raise any doubts that they had regarding each item.
The instrument was then administered to the final sample of participants in order to establish its validity. The data were collected from students of the University of Granada through stratified sampling by conglomerates, according to majors and groups of the different degrees taught at the University of Granada (Psychology, Speech Therapy, Tourism, English, History, Literature, GADE, Economy, Biology, Physics, Optics, Primary, Infant, Pedagogy, Law, Medicine, Pharmacy, Social Work, Policies, Sociology, Information Technology, Roads and Telecommunications). Teachers responsible for the selected groups were sent an email informing them of the objectives of the study and requesting their help so that the students could participate. They were asked to inform their students about the study and the time during breaks was used to complete the questionnaires. It was emphasized that the participation was voluntary, that is, the students were free not to participate if they preferred it.The teachers also emphasized the need for honesty when filling out the survey and guaranteed the confidentiality of the responses. The survey started with short demographic questions (sex and age) followed by the ATeMo questionnaire.
Data Analysis
To obtain empirical evidence about the construct validity of the questionnaire and given the ordinal nature of the data, we conducted Confirmatory Factor Analysis (CFA) using polychoric correlations and Unweighted Least Squares (ULS) as estimation method (Hernández et al., 2000; Yang-Wallentin et al., 2010; Morata-Ramírez et al., 2015). We also tested the basic psychometric properties of the dimensions obtained (mean, standard deviation, reliability and discrimination). For criterion validity, correlation analysis was performed to determine the relationship of the ATeMo factors and the sub-dimensions of the MULTICAGE CAD-4. Gender differences between the different factors of the questionnaire were also examined through a MANOVA. Finally, to achieve an initial approximate interpretation of the scores, we calculated the percentiles in the total sample and split them by gender. The statistical programs used were SPSS 15.0 for Windows and LISREL 8.71 (Jöreskog and Sörbom, 1996).
Results
Confirmatory Factor Analysis (CFA)
In order to obtain empirical evidence about the adequateness of the postulated structure ofthe ATeMo questionnaire, a CFA was conducted. In line with the theoretical background, the dimensional structure considered implied a general second-order factor referring to mobile phone dependence and four first order factors. The four first order factors were the following: eight items contributed to the first factor of Craving (1, 2, 3, 4, 9, 10, 12, 16), four items to the second factor of Loss of Control (5, 8, 13, 14), eight items to the third factor of Negative Life Consequences (6, 7, 11, 17, 18, 23, 24, 25) and five items to the fourth factor Withdrawal Syndrome (15, 19, 20, 21, 22). For the model examined (Figure 1), the Global fit Indices were: χ2 = 274.18; d.f. = 265; p = 0.34. The value of the Root Mean Square Error of Approximation (RMSEA) was 0.021, with a 90% interval between 0.0 and 0.050. The Goodness of Fit Index (GFI) was 0.97, the Adjusted Goodness of Fit Index (AGFI) was 0.97, the comparative Fit Index (CFI) was 1, the Normed Fit Index (NFI) was 1 and the Standardized Root Mean Square Residual (SRMR) was 0.06. These data show that the fit values of the model are appropriate. All the lambdas and gammas parameters were statistically significant.
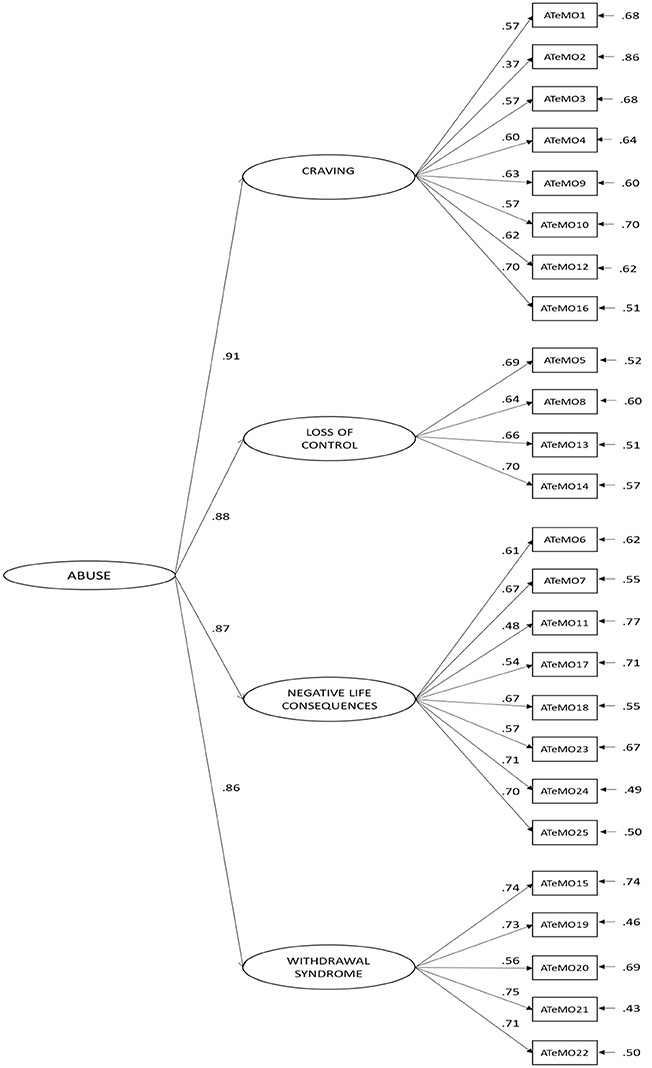
Figure 1. χ2 = 274.18; d.f. = 265; p = 0.34; RMSEA = 0.021, GFI = 0.97; AGFI = 0.97; CFI = 1; NFI = 1; and SRMR = 0.06.
Reliability
The reliability of ATeMo was assessed using Cronbach's alpha coefficients (Table 3) and the resulting values were: Total score 0.91; Craving factor 0.74; the Loss of Control factor 0.70; Negative Life Consequences factor 0.77; and for the Withdrawal Syndrome factor 0.77. In addition, we calculated descriptors for the ATeMo from the CFA (mean, standard deviation and mean discrimination of the items of each dimension: Table 2).
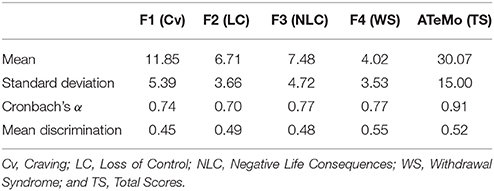
Table 2. Cronbach's alpha coefficients and the mean, standard deviation, and mean discrimination for the AteMo questionnaire derived from the CFA.
Criterion Validity
To determine the criterion validity, we calculated the Pearson bivariate correlation index between the total score and each of the ATeMo factors, as well as with the MULTICAGE CAD-4 subscales (see Table 3). There was a positive correlation between the ATeMo total score and Alcoholism, Gambling disorders, Internet addiction, and Compulsive buying in the MULTICAGE CAD-4 subscales. Furthermore, there was a positive correlation between the Negative Life Consequences factor of ATeMo and Drug addiction in the MULTICAGE CAD-4 subscale; the Craving and Loss of Control ATeMo factors and Video game addiction in the MULTICAGE CAD-4 subscale; and the Negative Life Consequences and Withdrawal Syndrome factors of ATeMo and Sex addiction in the MULTICAGE CAD-4 subscale.
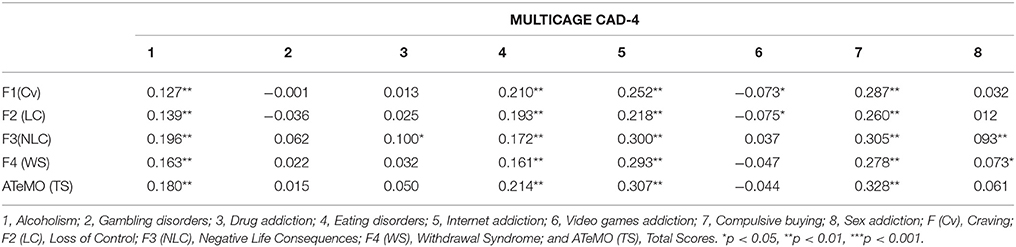
Table 3. Correlations between the total score, the factors of ATeMo, and the MULTICAGE CAD-4 subscales.
In general terms, the direction of the correlations is consistent with what was expected, however, given the large sample size, correlations of 0.073 (Craving-Video games addiction), for example, result statistically significant. For this reason, according to Rosnow and Rosenthal (1996) none of the correlations presents a large effect size (|r| > 0.37). The effect size is medium (|r| > 0.24) for the correlations between the factors of ATeMO with Internet Addiction, and Compulsive Buying. The correlation between the factors of ATeMO and Alcoholism and Eating Disorders have a low effect size (|r| > 0.10). All other correlations have an irrelevant effect size.
Score Interpretation
In order to provide preliminary data to help interpret the scores obtained, the 10th to 90th percentiles are presented for the total sample, and for men and women separately (Table 4).
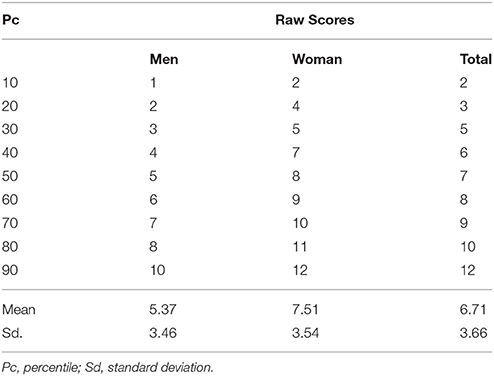
Table 4. Percentiles, raw scores in ATeMo, mean and standard deviation for men and women.
Discussion
In the present study we have developed a new valid and reliable scale to measure mobile phone abuse and dependence in Spain (ATeMo). The ATeMo Questionnaire consists of 25 items covering addictive symptoms, based on the diagnostic criteria of the DSM-5 (American Psychiatric Association, 2012). It is evaluated on a 5-point Likert-type scale ranging from 0 (strongly disagree) to 4 (agree), resulting in a final score in the range of 0–100. According to results from a confirmatory factor analysis, the ATeMo represents a general second order factor and four first order factors consistent with addiction theory: Craving, Loss of Control, Negative Life Consequences, and Withdrawal Syndrome. These factors show considerable overlap with the symptoms proposed previously (Bianchi and Phillips, 2005; Rutland et al., 2007; Igarashi et al., 2008; Yen et al., 2009; Walsh et al., 2010; Chóliz, 2012; Merlo et al., 2013; Chóliz et al., 2016) and were developed according to the criteria for the diagnostic symptoms of substance dependence disorders in the DSM-IV-TR (American Psychiatric Association, 2002) and the DSM-5 (American Psychiatric Association, 2012), the latter more recently including craving as a diagnostic criterion.
In assessing the reliability of the ATeMo questionnaire, Cronbach's alpha coefficients were calculated, demonstrating it had excellent internal consistency as seen elsewhere in similar studies in Spain (Chóliz, 2012; López-Fernández et al., 2012; Vanyukov et al., 2012; Chóliz et al., 2016). These coefficients were higher than those obtained in some previous studies (Fargues et al., 2009), where measures were developed according to the criteria for diagnosing symptoms of substance dependence disorders in DSM-IV-TR (American Psychiatric Association, 2002). The MULTICAGE CAD-4 subscales were used to determine potential criterion validity of ATeMo, identifying a positive correlation between the ATeMo total score and Alcoholism, Drug addiction, Eating disorders, Internet addiction, and Compulsive Buying subscales (Chiu et al., 2013; Gallimberti et al., 2016; Jiang and Shi, 2016; De-Sola et al., 2017a). Furthermore, there was a positive correlation between the Craving ATeMo factor, Alcoholism, Eating disorders, and Internet addiction, and a negative correlation with Video gaming addiction in the MULTICAGE CAD-4 subscale. Similarly, there was a positive correlation between the ATeMo factor Loss of Control and Alcoholism, Eating disorders, Internet addiction, and Compulsive buying, as well as a negative correlation with Gambling Disorders in the MULTICAGE CAD-4 subscale. This is consistent with the positive correlation between self-control and addiction identified previously (Jiang and Shi, 2016). Again, there was a positive correlation with Negative Life Consequences as an ATeMo factor and Alcoholism, Drug addiction, Eating disorders, Internet addiction, Compulsive buying, and Sex addiction in the MULTICAGE CAD-4 subscale, and there was a similarly positive correlation between Withdrawal Syndrome as an ATeMo factor and Alcoholism, Eating disorder, Internet addiction, Video gaming addiction, and Compulsive buying. Indeed, loss of control, negative life consequences and withdrawal syndrome were already considered as diagnostic criteria for addiction disorders prior to DSM-5 (American Psychiatric Association, 2012).
The relationships described above are consistent with previous considerations that alcohol consumption may predict problematic mobile phone use (De-Sola et al., 2017a). They are also consistent with previous results on the relationship between Internet and mobile phone addiction (Chiu et al., 2013) and with previous results suggesting common impulsive aspects between compulsive buying and mobile phone addiction (Jiang and Shi, 2016).
Furthermore, the survey conducted indicated a common continuum of substance abuse and behavioral addictions, as identified previously in surveys that focused on such co-morbidity (Chiu et al., 2013; Jiang and Shi, 2016; De-Sola et al., 2017a; although an association between eating disorders and mobile phone abuse is yet to be found). These results suggest that alcohol, drugs, and pathological gambling may not be the only crippling addictions. Addiction statistics are scarce because many destructive habits (such as gaming, shopping, sex, etc.) are not yet officially recognized as addictions, although they could be problematic for many reasons. Some of these involve the direct manipulation of pleasure through the consumption of products like in the case of drug use disorders and food-related disorders.
The results obtained with ATeMo indicate that there are gender differences between males and females regarding mobile phone abuse, with scores ≥8 for the former and ≥10 for the latter potentially indicating mobile phone addiction. These results are consistent with previous findings indicating that females send more and longer texts, they talk for longer than men on the phone, and tend to regard mobile phones as a social tool (Roberts et al., 2014).
Our findings demonstrate that the ATeMo is a valid and reliable instrument that can be administered to different groups of university students. In addition, while this instrument was developed for university students, renewed construct validity and reliability analyses could convert it into a version suitable for adolescents.
Our results should be evaluated in view of several important limitations. First, the sample used in this study was relatively homogeneous with respect to age and educational level. Second, mobile phone addiction should be investigated in relation to a number of variables, such as demographic, personality, and clinical characteristics. This could advance our understanding of the interaction of humans with technology, as well as our understanding of the nature and causes of technology-related addictions. Overall, taking into account the lack of a valid and reliable questionnaire to measure the addiction to the mobile phone, ATeMo could be an adequate instrument to measure the mobile phone addiction in future investigations.
Regarding clinical implications, the development of the ATeMo questionnaire to detect mobile phone abuse is an important step in the development of diagnostic and treatment procedures and in the design of prevention and intervention strategies.
In future studies, it would be of interest to examine the problems associated with mobile phone use in relation to variables such as solitude, depression, self-esteem, well-being, academic success, and other demographic variables. Further studies into the problematic use of mobile phones will not only allow us to better understand this problem but they should provide information to aid the committees determining future DSM criteria, especially in relation to addictions associated with new technologies. Moreover, a more profound analysis thorough ROC curves of the cut-off thresholds should be performed to help interpret the scores obtained and to classify the subjects. Moreover, other construct validity evidences should be investigated. In this sense, invariance analysis by gender, of age group, for example, is necessary to obtain empirical evidences about the equivalence in the constructs and items operatized in ATeMO. Once guarantee this issue, Differential Item Functioning and a deep comparative analysis by the sorting variables considered will be necessary to ensure that the decisions made based on the test scores are valid.
In summary, we have developed a scale to measure Mobile Phone Abuse, ATeMo, that takes into account the criteria for the diagnosis of substance use or addiction described in DSM-5 (American Psychiatric Association, 2002). The evaluation of craving was an important aspect of this questionnaire, as previously no measures existed that were consistent with the DSM-5 (American Psychiatric Association, 2012) criteria. The majority of measures had been developed based on the literature on substance use and addiction (Toda et al., 2004; Bianchi and Phillips, 2005; Rutland et al., 2007; Igarashi et al., 2008; Yen et al., 2009; Walsh et al., 2010; Chóliz, 2012; López-Fernández et al., 2012; Merlo et al., 2013; Chóliz et al., 2016), and the items in most of the previous instruments reflect the diagnostic criteria for substance use or addiction described in DSM-IV-TR (American Psychiatric Association, 2012). Based on the current findings we can conclude that the ATeMo questionnaire has satisfactory reliability and validity, having included craving as a diagnostic criteria for dependence.
Availability of Data and Materials
R code and data are available from the authors under request.
Ethics Statement
This study was approved by the Research Ethics Committee from the Granada University. All procedures performed in our study involving human participants were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants included in the study.
Author Contributions
All the authors participated in the conception and design of the work, specifically MO-C and FL-T, conceived the original idea for the study, obtained funding and wrote the study protocol. MO-C manages the day to day running of the study, including all participant follow-up and IR-U and PH-T undertaked all data analyses. This study paper was written by FL-T, IR-U, and PH-T with input from all co-authors. All authors read and approved the final manuscript and believe that the manuscript represents valid work; carefully read and fully approve of it.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
This research was supported by the Occupational Medicine Area (Prevention Service) of the University of Granada. We would like to thank all of the participant in this study.
References
Abebe, D. S., Hafstad, G. S., Brunborg, G. S., Kumar, B. N., and Lien, L. (2015). Binge drinking, cannabis and tobacco use among ethnic Norwegian and ethnic minority adolescents in Oslo, Norway. J. Immigr. Minor. Health 17, 992–1001. doi: 10.1007/s10903-014-0077-9
American Psychiatric Association (2012). DSM-5: The Future of Psychiatric Diagnosis. Available inline at: http://www.dsm5.org/Pages/Default.aspx
American Psychiatric Association (2002). Diagnostic and Statistical Manual of Mental Disorders IV-TR. Washington, DC: American Psychiatric Association.
Bianchi, A., and Phillips, J. G. (2005). Psychological predictors of problem mobile phone use. Cyberpsychol. Behav. 8, 39–51. doi: 10.1089/cpb.2005.8.39
Billieux, J., Gay, P., Rochat, L., and Van der Linden, M. (2010). The role of urgency and its underlying psychological mechanisms in problematic behaviours. Behav. Res. Ther. 48, 1085–1096. doi: 10.1016/j.brat.2010.07.008
Billieux, J., Philippot, P., Schmid, C., Maurage, P., De Mol, J., and Van, D. L. (2014). Is dysfunctional use of the mobile phone a behavioural addiction? Confronting symptom based versus process based approaches. Clin. Psychol. Psychother. 22, 460–468. doi: 10.1002/cpp.1910
Billieux, J., Van Der Linden, M., and Rochat, L. (2008). The role of impulsivity in actual and problematic use of the mobile phone. Appl. Cogn. Psychol. 22, 1195–1210. doi: 10.1002/acp.1429
Biolcati, R. (2015). Women between normality and dependence: a study of problematic consumption and dependence in women aged 30-50 years. J. Subst. Use 20, 143–150. doi: 10.3109/14659891.2013.878759
Blasco, J., Martínez-Raga, J., Carrasco, E., and Didia-Attas, J. (2008). Atención y craving o ganas compulsivas. Avances en su conceptualización y su implicación en la prevención de recaídas. Adicciones 20, 365–376.
Chiu, S. I., Hong, F. Y., and Chiu, S. L. (2013). An analysis on the correlation and gender difference between college students' internet addiction and mobile phone addiction in Taiwan. ISRN Addict. 2013:360607. doi: 10.1155/2013/360607
Chóliz, M. (2012). Mobile-phone addiction in adolescence: the test of mobile phone dependence (TMD). Prog. Health Sci. 2, 33–44.
Chóliz, M., Pinto, L., Phansalkar, S. S., Corr, E., Mujjahid, A., Flores, C., et al. (2016). Development of a Brief Multicultural Version of the Test of Mobile Phone Dependence (TMD brief) Questionnaire. Front. Psychol. 7:650. doi: 10.3389/fpsyg.2016.00650
Contreras-Rodríguez, O., Albein-Urios, N., Vilar-López, R., Perales, J. C., Martínez-González, J. M., Fernández-Serrano, M. J., et al. (2016). Increased corticolimbic connectivity in cocaine dependence versus pathological gambling is associated with drug severity and emotion-related impulsivity. Addict. Biol. 21, 709–718. doi: 10.1111/adb.12242
De-Sola, J., Talledo, H., Rubio, G., and de Fonseca, F. R. (2017a). Psychological factors and alcohol use in problematic mobile phone use in the Spanish population. Front. Psychiatry 8:11. doi: 10.3389/fpsyt.2017.00011
De-Sola, J., Talledo, H., Rubio, G., and de Fonseca, F. R. (2017b). Development of a mobile phone addiction craving scale and its validation in a spanish adult population. Front. Psychiatry 8:90. doi: 10.3389/fpsyt.2017.00090
Fargues, M. B., Lusar, A. C., Jordania, C. G., and Sánchez, X. C. (2009). Validación de dos escalas breves para evaluar la adicción a internet y el abuso de móvil. Psicothema 21, 480–485.
Fishman, J. A., and Galguera, T. (2003). Introduction to Test Construction in the Social and Behavioral Sciences. Lanham: Rowman And Littlefield Publishers, Inc.
Foerster, M., Roser, K., Schoeni, A., and Röösli, M. (2015). Problematic mobile phone use in adolescents: derivation of a short scale MPPUS-10. Int. J. Public 60, 277–286. doi: 10.1007/s00038-015-0660-4
Furr, M. (2011). Scale Construction and Psychometrics for Social and Personality Psychology. Los Angeles, CA: SAGE Publications.
Gallimberti, L., Buja, A., Chindamo, S., Terraneo, A., Marini, E., Rabensteiner, A., et al. (2016). Problematic cell phone use for text messaging and substance abuse in early adolescence (11- to 13-year-olds). Eur. J. Pediatr. 175, 355–364. doi: 10.1007/s00431-015-2645-y
Grant, J. E., Schreiber, L. R., and Odlaug, B. L. (2013). Phenomenology and treatment of behavioural addictions. Can. J. Psychiatry 58, 252–259. doi: 10.1177/070674371305800502
Ha, J. H., Chin, B., Park, D. H, Ryu, S. H., and Yu, J. (2008). Characteristics of excessive cellular phone use in korean adolescents. Cyber. Psychol. Behav. 11, 783–784. doi: 10.1089/cpb.2008.0096
Hernández, A., Muñiz, J., and García, E. (2000). Comportamiento del modelo de respuesta graduada en función del número de categorías de la escala. Psicothema 12, 288–291.
Igarashi, T., Motoyoshy, T., Takai, J., and Yoshida, T. (2008). No mobile, no life: Self-perception and text-message dependency among Japanese high school students. Comput. Hum. Behav. 24, 2311–2324. doi: 10.1016/j.chb.2007.12.001
Jenaro, C., Flores, N., Gómez-Vela, M., González-Gil, F., and Caballo, C. (2007). Problematic internet and cell-phone use: psychological behavioral, and health correlates. Addict. Res. Theory 15, 309–320. doi: 10.1080/16066350701350247
Jiang, Z., and Shi, M. (2016). Prevalence and co-occurrence of compulsive buying, problematic internet and mobile phone use in college students in Yantai, China: relevance of self-traits. BMC Public Health 16:1211. doi: 10.1186/s12889-016-3884-1
Jöreskog, K. G., and Sörbom, D. (1996). LISREL 8 User's reference guide. Chicago, IL: Scientific Software.
Kawasaki, N., Tanei, S., Ogata, F., Burapadaja, S., Loetkham, C., Nakamura, T., et al. (2006). Survey on cellular phone usage on students in thailand. J. Physiol. Anthropol. 25, 377–382. doi: 10.2114/jpa2.25.377
Kwon, M., Kim, D. J., Cho, H., and Yang, S. (2013). The smartphone addiction scale: development and validation of a short version for adolescents. PLoS ONE 8:83558. doi: 10.1371/journal.pone.0083558
Larsen, C. V. L., Curtis, T., and Bjerregaard, P. (2013). Harmful alcohol use and frequent use of marijuana among lifetime problem gamblers and the prevalence of cross-addictive behaviour among green land inuit: Evidence from the cross-sectional inuit health in transition green land survey 2006-2010. Int. J. Circumpolar Health 72, 1–9. doi: 10.3402/ijch.v72i0.19551
Lee, K., Lee, H. K., Gyeong, H., Yu, B., Song, Y. M., and Kim, D. (2013). Reliability and validity of the Korean version of the Internet Addiction Test among college students. J. Korean Med. Sci. 28, 763–768. doi: 10.3346/jkms.2013.28.5.763
Leeman, R. F., and Potenza, M. N. (2013). A targeted review of the neurobiology and genetics of behavioural addictions: an emerging area of research. Can. J. Psychiatry 58, 260–273. doi: 10.11772F070674371305800503
Leung, L. (2008). Linking psychological attributes to addiction and improper use of the mobile phone among adolescents in Hong Kong. J. Child Media 2, 93–113. doi: 10.1080/17482790802078565
Lin, T. T. C., Chiang, Y., and Jiang, Q. (2015). Sociable people beware? Investigating smartphone versus no smartphone dependency symptoms among young Singaporeans. Soc. Behav. Personal 43, 1209–1216. doi: 10.2224/sbp.2015.43.7.1209
López-Fernández, O., Honrubia-Serrano, M., and Freixa-Blanxart, M. (2012). Adaptación española del “Mobile Phone Problem Use Scale” para población adolescente. Adicciones 24, 123–130. doi: 10.20882/adicciones.104
López-Torrecillas, F., García, J., Godoy, J. F., García, M. P., Izquierdo, D. G., and Sánchez-Barrera, M. B. (2000). Variables modulating stress and coping that discriminate drug consumers from low or nondrug consumers. Addict. Behav. 25, 161–165. doi: 10.1016/S0306-4603(98)00121-X
Marlatt, G. A., Baer, J. S., Donovan, D. M., and Kivlahan, D. R. (1988). Addictive behaviors: etiology and treatment. Annu. Rev. Psychol. 39, 223–252.
Mattebo, M., Tydén, T., Häggström-Nordin, E., Nilsson, K. W., and Larsson, M. (2013). Pornography consumption, sexual experiences, lifestyles, and self-rated health among male adolescents in Sweden. J. Dev. Behav. Pediatr. 34, 460–468. doi: 10.1097/DBP.0b013e31829c44a2
Mentzoni, R. A., Brunborg, G. S., Molde, H., Myrseth, H., Skouverøe, K. J. M., Hetland, J., et al. (2011). Problematic video game use: estimated prevalence and associations with mental and physical health. Cyberpsychol. Behav. Soc. Netw. 14, 591–596. doi: 10.1089/cyber.2010.0260
Merlo, L. J., Stone, A. M., and Bibbey, A. (2013). Measuring problematic mobile phone use: Development and preliminary psychometric properties of the PUMP scale. J Addict. 2013:912807. doi: 10.1155/2013/912807
Míguez, C. M., and Becoña, E. (2015). Do cigarette smoking and alcohol consumption associate with cannabis use problem gambling among Spanish adolescents? Adicciones 27, 8–16.
Morata-Ramírez, M., Holgado-Tello, F., Barbero-García, I., and Mendez, G. (2015). Confirmatory factor analysis. Recommendations for unweighted least squares method related to Chi-Square and RMSEA. Accion Psicol. 12, 79–90. doi: 10.5944/ap.12.1.14362
Mudry, T. E., Hodgins, D. C., el-Guebaly, N., Cameron Wild, T., Colman, I. B., Schopflocher, D., et al. (2011). Conceptualizing excessive behaviour syndromes: a systematic review. Curr. Psychiatry Rev. 7, 138–151. doi: 10.2174/157340011796391201
Navas, J. F., Billieux, J., Perandrés-Gómez, A., López-Torrecillas, F., Cándido, A., and Perales, J. C. (2017). Impulsivity traits and gambling cognitions associated with gambling preferences and clinical status. Int. Gambl. Stud. 17, 102–124. doi: 10.1080/14459795.2016.1275739
Osuch, E., Vingilis, E., Ross, E., Forster, C., and Summerhurst, C. (2013). Cannabis use addiction risk and functional impairment in youth seeking treatment for primary mood or anxiety concerns. Int. J. Adolesc. Med. Health 25, 309–314. doi: 10.1515/ijamh-2013-0067
Pedrero-Pérez, E. J., Rodríguez-Monje, M. T., Gallardo- Alonso, F., Fernández- Girón, M., Pérez- López, M., and Chicharro- Romero, J. (2007). Validación de un instrumento para la detección de trastornos de control de impulsos y adicciones: el MULTICAGE CAD-4. TrastorAdic 9, 269–278. doi: 10.1016/S1575-0973(07)75656-8
Roberts, J. A., Petnji-Yaya, L. H., and Manolis, C. (2014). The invisible addiction: Cell-phone activities and addiction among male and female college students. J. Behav. Addict. 3, 254–265. doi: 10.1556/JBA.3.2014.015
Roser, K., Schoeni, A., Foerster, M., and Röösli, M. (2016). Problematic mobile phone use of Swiss adolescents: is it linked with mental health or behaviour? Int. J. Public Health 61, 307–315. doi: 10.1007/s00038-015-0751-2
Rosnow, R. L., and Rosenthal, R. (1996). Computing contrasts, effect sizes, and counternulls on other people's published data: general procedures for research consumers. Psychol. Methods 1, 331–340. doi: 10.1037/1082-989X.1.4.331
Ruiz-Olivares, R., Lucena, V., Pino, M. J., and Herruzo, J. (2010). Análisis de comportamientos relacionados con el uso/abuso de internet, teléfono móvil, compras y juego en estudiantes universitarios. Adicciones 22, 301–310. doi: 10.20882/adicciones.171
Rutland, J. B., Sheets, T., and Young, T. (2007). Development of a scale to measure problem use of short message service: the SMS problem use diagnostic questionnaire. Prog. Health Sci. 10, 841–843. doi: 10.1089/cpb.2007.9943
Ryu, Y. S., and Smith-Jackson, T. L. (2006). Reliability and Validity of the Mobile Phone Usability Questionnaire (MPUQ). J. Usab. Stud. 2, 39–53.
Schepers, J. (2009). Test Construction: Theory and practice. A Course for Beginners. Saarbrucken: VDM, Verlag Dr. Muller.
Schuster, R. M., Mermelstein, R., and Wakschlag, L. (2013). Gender-specific relationships between depressive symptoms, marijuana use, parental communication and risky sexual behavior in adolescence. J. Youth Adolesc. 42, 1194–1209. doi: 10.1007/s10964-012-9809-0
Takao, M., Takahashi, S., and Kitamura, M. (2009). Addictive personality and problematic mobile phone use. Cyberpsychol. Behav., 2, 501–507. doi: 10.1089cpb.2009.0022
The International Telecommunication Union (2016). Available online at: http://www.itu.int/en/ITU-D/Statistics/Documents/facts/ICTFactsFigures'2016.pdf
Toda, M., Monden, K., Kubo, K., and Morimoto, K. (2004). Cellular phone dependence tendency of female university students. JPN J. Hyg. 59, 383–386. doi: 10.1265/jjh.59.383
Van Rooij, A. J., Kuss, D. J., Griffiths, M. D., Shorter, G. W., Schoenmakers, M. T., and Mheen, V. D. (2014). The (co-)occurrence of problematic video gaming, substance use, and psychosocial problems in adolescents. J. Behav. Addict. 3, 157–165. doi: 10.1556/JBA.3.2014.013
Vanyukov, M. M., Tarter, R. E., Kirillova, G. P., Kirisci, L., Reynolds, M. D., Kreek, M. J., et al. (2012). Common liability to addiction and “gateway hypothesis”: theoretical, empirical and evolutionary perspective. Drug Alcohol Depend. 123, 3–17. doi: 10.1016/j.drugalcdep.2011.12.018
Verdejo-García, A., López-Torrecillas, F., Carmen, O. G., and Pérez-García, M. (2004). Clinical implications and methodological challenges in the study of the neuropsychological correlates of cannabis, stimulant, and opioid abuse. Neuropsychol. Rev. 14, 1–41. doi: 10.1023/B:NERV.0000026647.71528.83
Viola, T. W., Tractenberg, S. G., Wearick-Silva, L., de, O. R., Pezzi, J., and Grassi-Oliveira, R. (2014). Long-term cannabis abuse and early-onset cannabis use increase the severity of cocaine withdrawal during detoxification and rehospitalization rates due to cocaine dependence. Drug Alcohol Depend. 144, 153–159. doi: 10.1016/j.drugalcdep.2014.09.003
Vorspan, F., Mehtelli, W., Dupuy, G., Bloch, V., and Lépine, J. (2015). Anxiety and substance use disorders: co-occurrence and clinical issues. Curr. Psychiatry Rep. 17:4. doi: 10.1007/s11920-014-0544-y
Walsh, S. P., White, K. M., and Young, R. (2010). Needing to connect: the effect of self and others on young people's involvement with their mobile phones. Aust. J. Psychol. 62, 194–203. doi: 10.1080/00049530903567229
Walther, B., Morgenstern, M., and Hanewinkel, R. (2012). Co-occurrence of addictive behaviours: personality factors related to substance use, gambling and computer gaming. Eur. Addict. Res. 18, 167–174. doi: 10.1159/000335662
Weinstein, A., and Lejoyeux, M. (2015). New developments on the neurobiological and pharmaco-genetic mechanisms underlying internet and videogame addiction. Am. J. Addict. 24, 117–125. doi: 10.1111/ajad.12110
Xu, H., Wu, X., Lan, Y., and Chen, Y. (2008). Development of mobile phone dependence inventory for college students. Chin. J. Clin. Psychol. 16, 26–27.
Yang-Wallentin, F., Jöreskog, K. G., and Luo, H. (2010). Confirmatory factor analysis of ordinal variables with misspecified models. Struct. Equ. Model. 17, 392–423. doi: 10.1080/10705511.2010.489003
Yau, Y. H., Crowley, M. J., Mayes, L. C., and Potenza, M. N. (2012). Are Internet use and videogame-playing addictive behaviors? Biological, clinical and public health implications for youths and adults. Min. Psichiatr. 53, 153–170.
Keywords: mobile phone, DSM-5, validity, Spanish population, abuse
Citation: Olivencia-Carrión MA, Ramírez-Uclés I, Holgado-Tello P and López-Torrecillas F (2018) Validation of a Spanish Questionnaire on Mobile Phone Abuse. Front. Psychol. 9:621. doi: 10.3389/fpsyg.2018.00621
Received: 28 November 2017; Accepted: 12 April 2018;
Published: 30 April 2018.
Edited by:
Pietro Cipresso, Istituto Auxologico Italiano (IRCCS), ItalyReviewed by:
Juan Jose Fernandez Muñoz, Universidad Rey Juan Carlos, SpainStephane Rothen, Université de Genève, Switzerland
Roser Granero, Universidad Autónoma de Barcelona, Spain
Copyright © 2018 Olivencia-Carrión, Ramírez-Uclés, Holgado-Tello and López-Torrecillas. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Francisca López-Torrecillas, fcalopez@ugr.es