 Benjamin Rolland
Benjamin Rolland Mickael Naassila
Mickael Naassila Céline Duffau
Céline Duffau Hakim Houchi
Hakim Houchi Fabien Gierski
Fabien Gierski Judith André
Judith André- 1Groupe de Recherche sur l’Alcool & les Pharmacodépendances (GRAP), INSERM ERi 24, Centre Universitaire de Recherche en Santé, Université de Picardie Jules Verne, Amiens, France
- 2C2S Laboratory (EA 6291), University of Reims Champagne-Ardenne, Reims, France
Many studies have suggested the co-occurrence of eating disorders and alcohol use disorders but in which extent binge eating (BE) and other disordered eating symptoms (DES) are associated with the severity of binge drinking (BD) remains unknown. We conducted a online cross-sectional study among 1,872 French students. Participants were asked their age, gender, tobacco and cannabis use status. They completed the Alcohol Use Questionnaire (AUQ), Eating Disorder Examination Questionnaire (EDE-Q), and UPPS impulsive behavior questionnaire. BD score was calculated using the AUQ. Three items of the EDE-Q were used to construct a BE score. The predictors of the BD score were determined using a linear regression model. Our results showed that the BE score was correlated with the BD score (β0 = 0.051 ± 0.022; p = 0.019), but no other DES was associated with BD, including purging behaviors. The severity of BD was also correlated with younger age, male gender, tobacco and cannabis use, and with the ‘positive urgency,’ ‘premeditation,’ and ‘sensation seeking’ UPPS subscores (R2 of the model: 25%). Within DES, BE appeared as an independent determinant of the BD severity. This is in line with the recent hypothesis that BE is not a subtype of DES, but more a general vulnerability factor of emotional dysregulation, which could be shared by different behavioral and addictive disorders.
Introduction
Alcohol use disorders (AUDs) (alcohol abuse and addiction) often co-occur with eating disorders. Bulimia nervosa and bulimic behaviors, binge eating (BE), purging, anorexia nervosa and atypical eating disorders have been associated with AUDs in women in a meta-analysis study (Gadalla and Piran, 2007; Baker et al., 2010; Root et al., 2010).
Binge drinking (BD) consists of episodic heavy alcohol drinking, and is often associated with drunkenness-oriented alcohol use1. Similarly, BE has been defined in the DSM-5 as abnormal eating episodes, which comprise eating much more rapidly or much larger amounts of food than normal, eating alone because of being embarrassed by how much one is eating, and feeling disgusted with oneself, depressed, or guilty after overeating.
Common cognitive and behavioral features have been described, and common integrative models have been proposed, with regard to BD and BE (Ferriter and Ray, 2011). BD and BE may share several features, such as repetitive engagement in the behavior despite evidence negative consequences (physical problems and poor academic performance), personality correlate such as neuroticism, and affected characteristics such as elevated levels of negative affect (impulsivity, anxiety, and depression). Concerning the common explanatory models of BD and BE, existing research proposed several key models such as the basic functional model, the motivational model, the expectancies model and the craving model (Ferriter and Ray, 2011).
Nevertheless, the possible interrelationships between BD and BE have only started to be explored. A couple of previous studies found frequent prevalence association between BE and BD, especially in women (Luce et al., 2007; Khaylis et al., 2009). However, though a characterized BE disorder has been defined by the DSM-5, BD remains a very heterogeneous set of drinking behaviors, with multiple and sometimes-questioned official definitions (Courtney and Polich, 2009). In many epidemiological studies, BD is frequently investigated by delineating populations using a cut-off drinking threshold (Courtney and Polich, 2009), which mixes BD subjects into a same group, and makes hard to address severity factors. For example, according to the World Health Organization (WHO), BD is defined as consuming at least 60 g of alcohol per drinking episode but some subjects drink at levels far beyond this binge threshold making difficult the study of severity aspects. That is why some authors have proposed using BD severity scores (Townshend and Duka, 2005). The BD score founded on patterns of drinking, rather than only quantities of alcohol consumed, may be more relevant of BD behavior.
In a more than 1800-subject sample of French students, we scored both BE and BD, as well as other DES, and we analyzed in which extent the BD score was determined by the scores of BE and other DES. It has never been assessed whether BE, as well as other disordered eating symptoms (DES), were associated with BD, not in terms of co-occurrence frequency, but as a specific severity factor of BD. In addition, since impulsivity has been consistently linked to the development and expression of BE and BD behaviors we assessed impulsivity behavior that may represent a common vulnerability factor.
Materials and Methods
Study Design and Participants
The study was an online anonymous survey conducted among all the students attending the French University of Rennes 1 in year 2012. 29,000 Students were invited to complete the questionnaire via their individual university email address. Students of Rennes 1 university are distributed as follows: 39% law, economy, management and human sciences, 28% health, 33% sciences, engineering and technologies. The link into the study could be activated only once, to avoid multiple participations in the survey. The identity of the participants completing the anonymous questionnaire was unknown to the researcher. No written informed consent was asked to the participants and the researcher’s contact information was indicated in the questionnaire. Students were able to continue with the survey only if they stated that they do consent to participate by ticking the consent button after reading the consent form (purpose of research, participation, procedure, confidentiality, and researcher’s contact information). Raw data were stored on a computer not connected to an internet network and were destroyed at the end of the study. The protocol was approved by the regional ethics committee (Comité de Protection des Personnes Nord-Ouest II).
Questionnaire and Type of Data Collected
Participants were asked to provide their age, gender, weight, height, current tobacco smoking status, and current cannabis use status. They were also invited to complete online versions of the Alcohol Use Questionnaire (AUQ) (Mehrabian and Russell, 1978), the Eating Disorder Examination Questionnaire (EDE-Q) (Fairburn and Beglin, 1994), and the 20-item Urgency – Premeditation – Perseverance – Sensation seeking (UPPS) impulsive behavior questionnaire (Billieux et al., 2012).
Score Construction
A BD score was calculated on the basis of three items of the AUQ, as previously validated (Townshend and Duka, 2005). The BD score was calculated for all participants on the basis of the information given in items 10, 11, and 12 of the AUQ [Speed of drinking (average drinks per hour); number of times being drunk in the previous 6 months; percentage of times getting drunk when drinking (average)]. The BD score is calculated as follows [4 × (Item 10) + Item 11 + 0.2 × (Item 12)]. This score gives a picture of the drinking patterns of the participants rather than just a measure of alcohol intake. Using the UPPS questionnaire, scores of ‘negative urgency,’ ‘positive urgency,’ ‘lack of premeditation,’ ‘lack of perseverance,’ and ‘sensation seeking’ were calculated for each participant (Billieux et al., 2012). Moreover, the Body Mass Index (BMI) of respondents was calculated on the basis of their reported weight and height. Using the EDE-Q questionnaire, scores of ‘dietary restraint,’ ‘eating concern,’ ‘shape concern,’ and ‘weight concern’ were calculated as defined by the authors of the questionnaire (Fairburn and Beglin, 1994). In addition, a BE score was calculated by summing the subscores of the items 13, 14, and 15, of the EDE-Q, while a ‘purging behaviors’ score was obtained by summing the specific questions of the EDE-Q, i.e., questions 16 and 17. Moreover, categorical BMI groups were constructed. All the subjects with a BMI of less than 18.5 were defined as the ‘underweight’ group. The ‘≥18.5 to <25’ group was defined as ‘normal,’ while the ‘≥25 group’ was defined as the ‘overweight’ group.
Statistical Analysis
Categorical variables are provided as the number and percentage (n; %). Quantitative variables are provided as the mean and standard deviation, and median and interquartile range (mean ± SD; med [IQR]). For both the BD and BE scores, bivariate analyses were conducted to explore the association with the other parameters explored. Comparisons between two quantitative measures were performed using the Spearman’s ρ test, whereas comparisons between quantitative and categorical variables were performed using Mann–Whitney or Kruskal–Wallis tests.
Furthermore, a multivariable linear regression modeling was built, with the BD score as the dependent variable, and other variables as the explanatory variables. The standardized coefficients of the model are provided with their standard deviation (β0 value ± SD). The significance threshold was fixed at 0.05 for all tests. Analyses were conducted using the XLSTAT2014 software2.
Results
Of the 29,000 students who were invited to complete the online questionnaire, 1,872 accepted to participate (mean age = 21.1 ± 2.44 years; median age = 21 [20–23]); 57.4% females; 21.4% tobacco smokers; 29.6% cannabis users).
Results of the bivariate comparisons of the BD and BE scores with other variables provided in the Table 1.
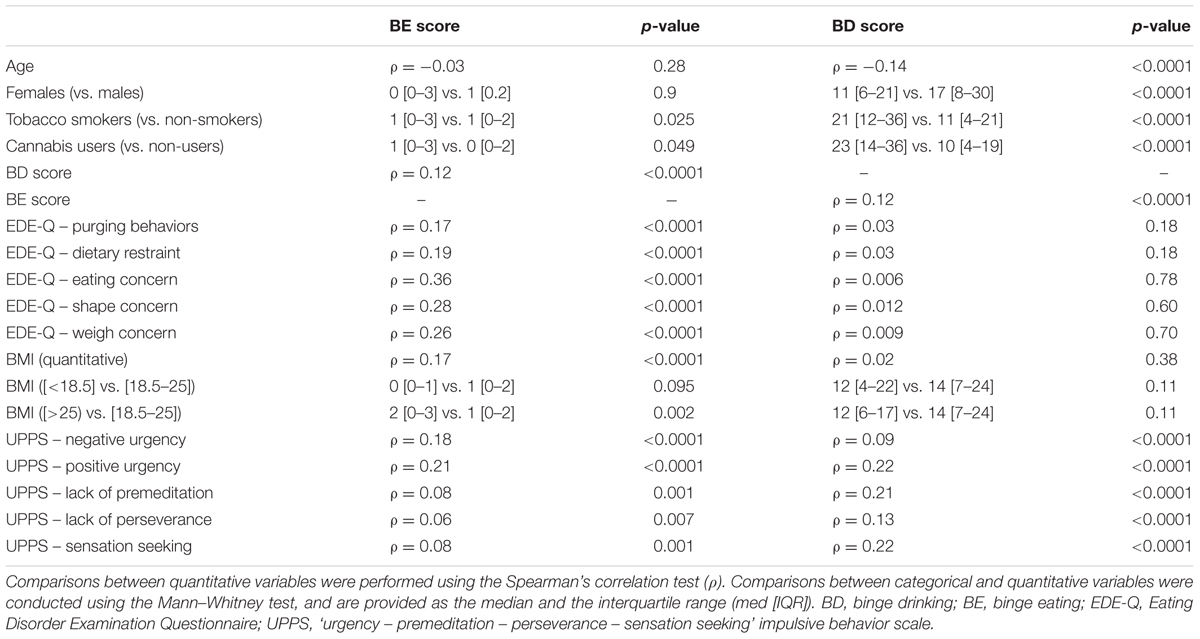
TABLE 1. Bivariable comparisons for the BE and BD scores.
The BD score was significantly associated with the BE score (ρ = 0.12; p < 0.0001), but not with other EDE-Q subscores. The BD score was also significantly associated with male gender (p < 0.0001), tobacco smoking status (p < 0.0001), and cannabis use status (p < 0.0001). It was also significantly correlated with every UPPS subscore (p < 0.0001 for each), and negatively associated with age (ρ = -0.14; p < 0.0001). Consequently, all these parameters were integrated in the multivariable linear regression model, which is provided in the Table 2.
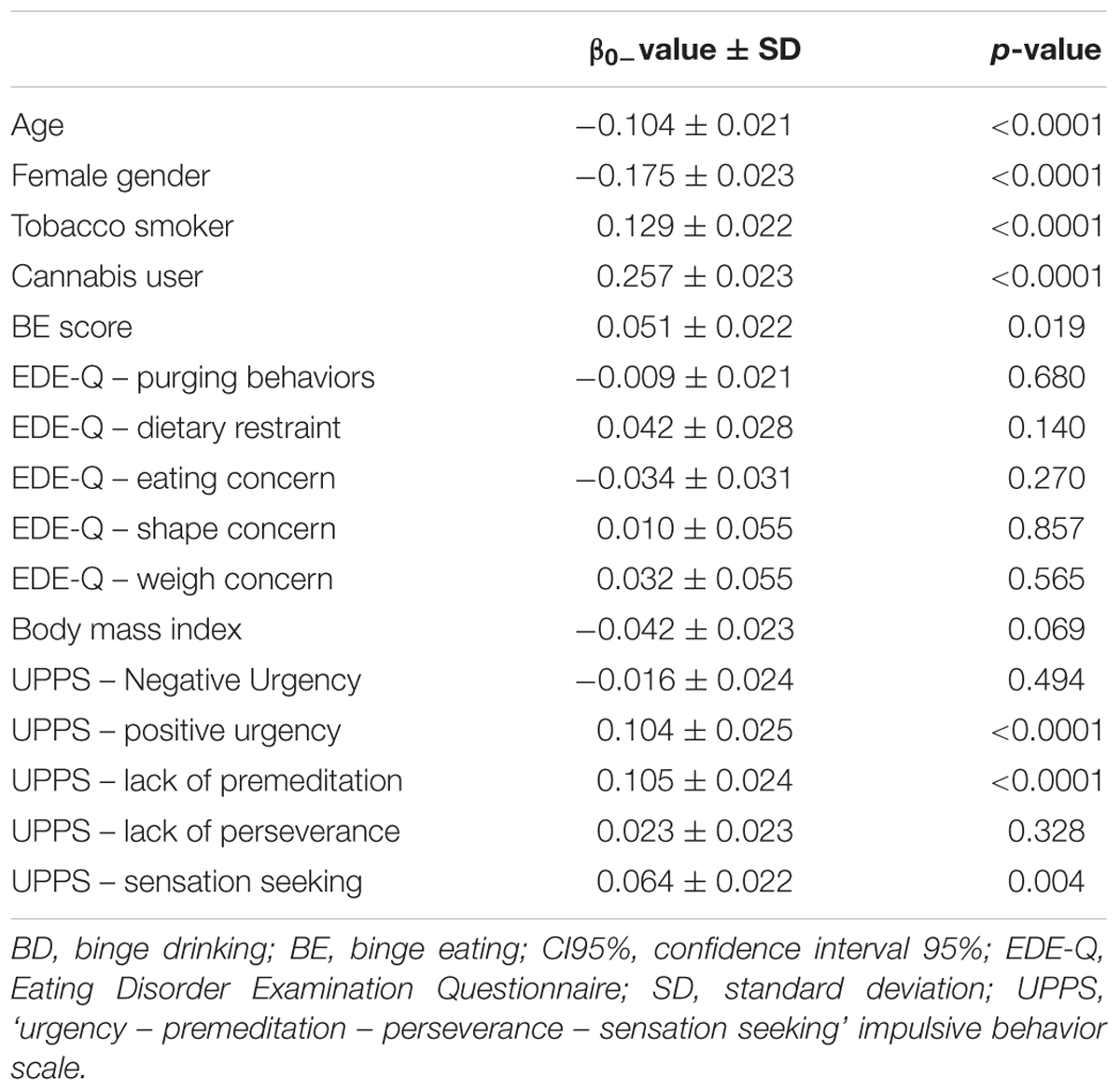
TABLE 2. Results of the multivariable linear regression modeling of the BD score (β0 = normalized coefficients; R2 = 25%).
In the multivariable modeling, the BE score remained significantly correlated with the BD score (β0-value = 0.051 ± 0.022; p = 0.019), whereas the scores of other DES were not significantly associated with the BD score. Male gender, younger age, tobacco smoking status, and cannabis use status, were all significant contributors of the BD score (p < 0.0001 for each parameter). In addition, only the ‘positive urgency’ (p > 0.0001), ‘lack of perseverance’ (p < 0.0001), and ‘sensation seeking’ (p = 0.004) subscores of the UPPS scale were significantly associated with the BD score. The overall goodness of fit of the model was R2 = 25%.
Discussion
The main objective of the study was to assess in which extent the different DES were significant contributors of the severity of BD in a population of French students. In this respect, we found that only the severity of BE, and not other dimensions of disordered eating, was significantly correlated to the BD score. Moreover, the BE score appeared also significantly correlated with all other EDE-Q subscores and with the BMI, whereas these different quantitative parameters were not correlated with the BD score.
These findings are consistent with some recent hypotheses, according to which BE should not be viewed as a subcategory of DES, but as the more general expression of an impaired emotion regulation, which would constitute a common vulnerability factor for eating disorders, as well as other addictive behaviors (Stojek et al., 2014; Leehr et al., 2015; Eichen et al., 2016). Impulsivity has been regularly, though inconstantly, associated with this BE-related emotional dysregulation (Schag et al., 2013; Stojek et al., 2014; Eichen et al., 2016). Consequently, it was important to adjust our analyses using impulsivity traits assessment to explore the severity of BD. However, this did not change our main results. Moreover, differentiating between BE and purging behaviors was never previously addressed in previous research on eating behaviors. In this regard, we found that purging behaviors, though highly associated with BE, were not associated with BD. To our knowledge, this is a second original finding.
Furthermore, our results are in line with several previous findings. ‘Positive urgency’ and ‘sensation seeking’ were both associated with substance use (Billieux et al., 2012), whereas ‘negative urgency’ was more associated with substance dependence (Verdejo-García et al., 2007). In our study, which did not focus on dependent subjects, we found a significant association between the BD score and the ‘positive urgency’ and ‘sensation seeking’ subscores of the UPPS. Moreover, previous investigations reported an association between BE and either ‘negative urgency’ (Bardone-Cone et al., 2016), or both ‘negative’ and ‘positive’ urgency dimensions (Stojek et al., 2014). In our study, we confirmed these associations, as, among all the UPPS subscores, both urgency subscores were those which showed the strongest association with the BE score.
Several limitations should also be acknowledged regarding this study. First and foremost, the response rate was only about 6.4% and can be partially explained by the fact that the majority of students do not use the email address provided by the university [but is not very low compared to that of similar studies (Tavolacci et al., 2016)]. We cannot exclude that the more involved or problematic individuals refused to participate and the lack of psychiatric interview is also an important limitation here since we did not detect the presence of psychiatric diagnosis in our sample. The entirely self-report dimension of the data analyzed may have impacted the reliability of the data despite the large sample size recruited and it has been already shown that for alcohol consumption, it may be underestimated by the use of retrospective questionnaire (Townshend and Duka, 2002), the self-report ascertainment of cannabis use may also be affected by the fact that some cannabis users may deny using cannabis.
The building of the BD score followed a validated procedure (Townshend and Duka, 2005) while the way the BE and purging scores were constructed was not based on previous studies. The global EDE-Q score has shown good psychometric properties to measure BE (Vander Wal et al., 2011), but no specific study has ever demonstrated the validity of the items we selected to, respectively, score the BE and purging behaviors. However, these items specifically focus on BE or purging symptoms. It is noteworthy that ‘purging behavior’ is not only defined by vomiting and laxative misuse (as highlighted in the EDE-Q) but also by other behaviors such as misuse of diuretics, infusions and sugar-free candies. Another possible limitation of the study is that no association was found between the female gender and the BE score, whereas BE is usually much more frequent among females (Allen et al., 2014). However, in the present study, we did not use a frequency but a severity assessment, which is not similar. The lack of between-gender difference would be questionable if BE would have been more severe among women, and not only more frequent. To our knowledge, this has not been demonstrated yet.
Conclusion
Overall, we found that the BE severity was correlated with the BD severity, contrary to other DES. These results suggest that BE could consist of a general vulnerability factor, underlying elements of emotional dysregulation that remain to be more understood. This common vulnerability could link different types of behaviors and mental disorders, which may elsewhere be poorly interrelated, like, in our study, BD and DES.
Author Contributions
MN and JA developed the study. All authors contributed to the study design. Data collection was conducted by CD and JA and data analyses were performed in collaboration with all authors (BR, MN, CD, HH, FG, and JA). BR drafted the paper under the supervision of MN, while HH, FG, and JA provided critical revisions. All authors approved the final version of the paper.
Funding
Both BR and MN received grants from the Fondation Actions-Addictions.
Conflict of Interest Statement
BR has provided expert testimony for Ethypharm and Indivior. And received lecture fees from Ethypharm, Lundbeck, Indivior, Bouchara-Recordati, Gilead, AstraZeneca, Bristol-Myers-Squibb, Otsuka, and Servier. MN received lecture or expert fees from Merck-Serono, Lundbeck and Bouchara-Recordati. Both BR and MN received grants from the Fondation Actions-Addictions. These funds did not exert any editorial direction or censorship on any part of this article. JA, HH and FG have no conflict of interest to declare regarding the present article. The other authors have no conflict of interest to declare regarding the present article.
Acknowledgments
The work provided by BR on this study was supported by a research grant from the Fondation Actions-Addictions (http://actions-addictions.org), which is an independent French foundation supporting evidenced-based actions against addictive disorders.
Footnotes
- ^ National Institute on Alcohol Abuse and Alcoholism (NIAAA). Drinking Levels Defined n.d. https://www.niaaa.nih.gov/alcohol-health/overview-alcohol-consumption/moderate-binge-drinking (accessed August 8, 2016).
- ^ https://www.xlstat.com/en/
References
Allen, K. L., Byrne, S. M., Oddy, W. H., Schmidt, U., and Crosby, R. D. (2014). Risk factors for binge eating and purging eating disorders: differences based on age of onset. Int. J. Eat. Disord. 47, 802–812. doi: 10.1002/eat.22299
Baker, J. H., Mitchell, K. S., Neale, M. C., and Kendler, K. S. (2010). Eating disorder symptomatology and substance use disorders: prevalence and shared risk in a population based twin sample. Int. J. Eat. Disord. 43, 648–658. doi: 10.1002/eat.20856
Bardone-Cone, A. M., Butler, R. M., Balk, M. R., and Koller, K. A. (2016). Dimensions of impulsivity in relation to eating disorder recovery. Int. J. Eat. Disord. 49, 1027–1031. doi: 10.1002/eat.22579
Billieux, J., Rochat, L., Ceschi, G., Carré, A., Offerlin-Meyer, I., Defeldre, A. C., et al. (2012). Validation of a short French version of the UPPS-P impulsive behavior scale. Compr. Psychiatry 53, 609–615. doi: 10.1016/j.comppsych.2011.09.001
Courtney, K. E., and Polich, J. (2009). Binge drinking in young adults: data, definitions, and determinants. Psychol. Bull. 135, 142–156. doi: 10.1037/a0014414
Eichen, D. M., Chen, E. Y., Schmitz, M. F., Arlt, J., and McCloskey, M. S. (2016). Addiction vulnerability and binge eating in women: exploring reward sensitivity, affect regulation, impulsivity & weight/shape concerns. Pers. Individ. Dif. 100, 16–22. doi: 10.1016/j.paid.2016.03.084
Fairburn, C. G., and Beglin, S. J. (1994). Assessment of eating disorders: interview or self-report questionnaire? Int. J. Eat. Disord. 16, 363–370.
Ferriter, C., and Ray, L. A. (2011). Binge eating and binge drinking: an integrative review. Eat. Behav. 12, 99–107. doi: 10.1016/j.eatbeh.2011.01.001
Gadalla, T., and Piran, N. (2007). Co-occurrence of eating disorders and alcohol use disorders in women: a meta analysis. Arch. Womens Ment. Health 10, 133–140. doi: 10.1007/s00737-007-0184-x
Khaylis, A., Trockel, M., and Taylor, C. B. (2009). Binge drinking in women at risk for developing eating disorders. Int. J. Eat. Disord. 42, 409–414. doi: 10.1002/eat.20644
Leehr, E. J., Krohmer, K., Schag, K., Dresler, T., Zipfel, S., and Giel, K. E. (2015). Emotion regulation model in binge eating disorder and obesity–a systematic review. Neurosci. Biobehav. Rev. 49, 125–134. doi: 10.1016/j.neubiorev.2014.12.008
Luce, K. H., Engler, P. A., and Crowther, J. H. (2007). Eating disorders and alcohol use: group differences in consumption rates and drinking motives. Eat. Behav. 8, 177–184. doi: 10.1016/j.eatbeh.2006.04.003
Mehrabian, A., and Russell, J. A. (1978). A questionnaire measure of habitual alcohol use. Psychol. Rep. 43, 803–806. doi: 10.2466/pr0.1978.43.3.803
Root, T. L., Pisetsky, E. M., Thornton, L., Lichtenstein, P., Pedersen, N. L., and Bulik, C. M. (2010). Patterns of co-morbidity of eating disorders and substance use in Swedish females. Psychol. Med. 40, 105–115. doi: 10.1017/S0033291709005662
Schag, K., Schönleber, J., Teufel, M., Zipfel, S., and Giel, K. E. (2013). Food-related impulsivity in obesity and binge eating disorder - a systematic review. Obes. Rev. 14, 477–495. doi: 10.1111/obr.12017
Stojek, M. M., Fischer, S., Murphy, C. M., and MacKillop, J. (2014). The role of impulsivity traits and delayed reward discounting in dysregulated eating and drinking among heavy drinkers. Appetite 80, 81–88. doi: 10.1016/j.appet.2014.05.004
Tavolacci, M. P., Boerg, E., Richard, L., Meyrignac, G., Dechelotte, P., and Ladner, J. (2016). Prevalence of binge drinking and associated behaviours among 3286 college students in France. BMC Public Health 16:178. doi: 10.1186/s12889-016-2863-x
Townshend, J. M., and Duka, T. (2002). Patterns of alcohol drinking in a population of young social drinkers: a comparison of questionnaire and diary measures. Alcohol Alcohol. 37, 187–192. doi: 10.1093/alcalc/37.2.187
Townshend, J. M., and Duka, T. (2005). Binge drinking, cognitive performance and mood in a population of young social drinkers. Alcohol. Clin. Exp. Res. 29, 317–325. doi: 10.1097/01.ALC.0000156453.05028.F5
Vander Wal, J. S., Stein, R. I., and Blashill, A. J. (2011). The EDE-Q, BULIT-R, and BEDT as self-report measures of binge eating disorder. Eat. Behav. 12, 267–271. doi: 10.1016/j.eatbeh.2011.07.006
Keywords: binge drinking, binge eating, binge-eating disorder, alcohol drinking, adolescent
Citation: Rolland B, Naassila M, Duffau C, Houchi H, Gierski F and André J (2017) Binge Eating, But Not Other Disordered Eating Symptoms, Is a Significant Contributor of Binge Drinking Severity: Findings from a Cross-Sectional Study among French Students. Front. Psychol. 8:1878. doi: 10.3389/fpsyg.2017.01878
Received: 24 June 2017; Accepted: 10 October 2017;
Published: 30 October 2017.
Edited by:
Salvatore Campanella, Université Libre de Bruxelles, BelgiumReviewed by:
Elena Tenconi, Università degli Studi di Padova, ItalyThomas Edward Gladwin, University of Chichester, United Kingdom
Copyright © 2017 Rolland, Naassila, Duffau, Houchi, Gierski and André. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mickael Naassila, mickael.naassila@inserm.fr