
Abstract
This paper evaluates the content of the syllabi of postgraduate courses on public health ethics (PHE) within accredited schools and programs of public health (PH) in the United States in order to gain an awareness of the topics addressed within these courses. Methods: Data was gathered via the analysis of syllabi of courses on PHE. In 2012, information was requested by e-mail from the 48 schools and 86 PH programs accredited by the U.S. Council on Education for Public Health for 2012. The “Epidemiology and PHE Syllabi” project of the University of Miami also was consulted. A table of topics was drawn up in order to carry out content analysis of the documents. Results: Data was obtained from 25 schools (52%) and 36 accredited programs (42%); 36 syllabi were gathered and 75 different topics were found. Of these, 38 topics were addressed in six or more syllabi and can be grouped as follows: foundations of PHE; autonomy and its limits; infectious disease control; justice; research ethics; health education and promotion; environmental and occupational health; screening; genetics; privacy and confidentiality; and community-based practice and vulnerable populations. Conclusions: The analyzed syllabi show high variability in curricular content. The debate with regard to whether a core curriculum on PHE should be established is ongoing. The results of this work might be of interest for schools and programs of PH in other countries or regions of the world in order to develop or ameliorate their own PHE syllabi.
Similar content being viewed by others

Introduction
The historical development of bioethics has been fundamentally linked to the fields of clinical health care and biomedical research (Rothman 1991). It was only in the 1980s, with the explosion of the AIDS epidemic, that this situation began to change (Bayer and Gostin 1990). Thus, during the 1990s, interest in public health ethics (PHE) grew slowly, sometimes dealing exclusively with epidemiology and on other occasions developing under the umbrella of broader debates (Coughlin and Beauchamp 1996; Bayer and Fairchild 2004). Most of these debates arose as a result of AIDS, such as the debate on the relationship between ethics, public health (PH), and human rights, which remains ongoing (Mann 1997; Gostin 2001; Cotter et al. 2009). However, it was not until the years between 1999 and 2002 that a broader perspective emerged in the United States, and a number of articles and books issued in that time are still considered to be cornerstones within this area of bioethics (Beauchamp and Steinbock 1999; Kass 2001; Gostin 2000; Bradley and Burls 2000; Childress et al. 2002; Callahan and Jennings 2002; Gostin 2002). Furthermore, 2002 saw the publication of the “Principles of the Ethical Practice of Public Health” (American Public Health Association 2002). These principles were subsequently adopted as a code of ethics by the American Public Health Association (Thomas et al. 2002).
Both the need to introduce ethics in the training curriculum of PH specialists in the United States and the difficulties involved had already been highlighted in studies before 2002 (Bluestone 1976; Coughlin, Katz, and Mattison 1999; Goodman and Prineas 1996; Coughlin 2000). Thus, when the Institute of Medicine (IOM) published its report entitled “Who Will Keep the Public Healthy?” in November 2002, ethics was identified as a priority issue (Gebbie, Rosenstock, and Hernandez 2003). This report entailed a review of the teaching of PH in the United States and indicated eight areas that should be particularly reinforced within the country’s schools and programs of PH. As we have already mentioned, PHE was one of these key areas.
Only a few months later, in July 2003, another document appeared proposing improvements in the field. It was entitled “Ethics and Public Health: Model Curriculum” (Jennings et al. 2003). This report was the result of a cooperative project involving the Association of Schools of Public Health (ASPH), the University of Minnesota Center for Bioethics, and The Hastings Center. Shortly after, in 2004, a document was published by the Public Health Leadership Society entitled “Skills for the Ethical Practice of Public Health” (Thomas 2004). This document was prepared by the North Carolina School of Public Health. It proposed five general competencies and a further 68 specific competencies grouped around the aforementioned 12 “Principles of the Ethical Practice of Public Health.” Thus, toward 2005, PH in the United States already had enough theoretical tools to systematically incorporate the teaching of PHE into its training programs: theoretical foundations, curricular proposals, and defined competencies.
The situation was very different in Europe. In 2003, Kessel—after mailing a questionnaire survey of the nature and content of teaching of PHE in the United Kingdom—found that 52 percent of institutions providing postgraduate education that filled in the questionnaire were teaching PHE (Kessel 2003). But the content and nature of this teaching is described by this author as “patchy and often minimal.” In 2010, a survey targeting the 82 members of the Association of Schools of Public Health in the European Region (ASPHER) was implemented (Aceijas et al. 2012).
As the authors point out,
the survey achieved a general response rate of 52.4 percent (n = 43/82) of which 40 (49.4 %) offered information on all three questionnaire sections revealing that 95 percent of the respondent schools included the teaching of ethics in at least one of its programmes (n = 38/40), 16 (39.02 %) in their bachelor programmes and in 38 (95 %) in their master programmes (Aceijas et al. 2012, 5).
Unfortunately, no evaluation of the topics included in the teaching was made but, significantly, all respondents “indicated that they wished to be supported by ASPHER for the ethics content of their Public Health programmes” (Aceijas et al. 2012, 7). The European Public Health Association (EUPHA) and ASPHER have established a joint working group to develop a core curriculum on PHE for the European region and they have a work in progress (Report of the ASPHER–EUPHA 2012). This fact suggests that PHE teaching is still in process of development in Europe.
This paper aims to contribute to ascertaining the degree to which the tools that PHE has developed in the United States have been applied in schools and programs of PH. The extent to which the competencies in PHE have been incorporated into the teaching programs in the United States has recently been examined (Lee, Wright, and Semaan 2013). This article, therefore, will focus on a description of the curricular content of these teaching programs via an analysis of the content of the syllabi of the specific courses on PHE. The information obtained can be useful for schools and programs of PH in other countries or regions of the world in order to develop or ameliorate their own PHE syllabi.
Methods
Over the course of November and December 2012, information was requested on the teaching of ethics in public health from the 48 U.S. schools of public health and 86 U.S. public health programs accredited in 2012 by the Council on Education for Public Health (Council on Education for Public Health 2012). An e-mail was sent to the deans of the schools and the directors of the programs, asking them whether any specific course on PHE had been taught or programmed for postgraduates (master’s students) during 2011 and 2012 or programmed for 2013 in their institution. Where this proved to be the case, they were asked to send the syllabus of the course in order to enable us to analyze its content. Two e-mails were sent, the first requesting the information and the second as a reminder two or three weeks later.
As an additional source of information on syllabi addressing PHE, data from the “Epidemiology and Public Health Ethics Syllabi” project, one of the University of Miami Ethics Programs, was consulted (University of Miami Ethics Programs. n.d.). This project aims to gather syllabi for courses in ethics in epidemiology and public health and is supported by the American College of Epidemiology. Syllabi of courses taught in 2011 or 2012 in accredited schools or programs were sought.
Analysis
The study of the syllabi was carried out using a document analysis methodology that combined an initial qualitative approach and a subsequent quantitative approach. In the initial qualitative phase, the two researchers (PSL and IMBC) separately analyzed each syllabus in order to draw up a list of the teaching topics included and, subsequently, compile a general list. To this end, the following sections were analyzed: objectives of the course (general and specific aims of each lesson), titles of the lessons, titles in the assigned reading lists for each lesson (required and recommended), and case studies proposed. It was therefore assumed that while a topic did not appear directly in the title of a lesson, it could be deduced that the teacher wished to introduce it and deal with it more indirectly through the required or recommended reading lists or via case studies. Subsequently, both lists were combined, enabling the fusion of similar topics, supplementing one list with the other until a single list was created that both researchers agreed upon. In the subsequent quantitative phase, using the aforementioned list as a checklist, each researcher evaluated all of the documents again in order to identify those that contained each of the topics on the list. Once again, both numerical tables were compared and all discrepancies between the two researchers were resolved, enabling the generation of a consensus on the final results.
Results
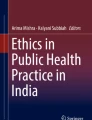
A total of 20 schools (response rate 42 percent) and 34 programs (response rate 40 percent) provided information on PHE syllabi (Fig. 1). Finally, taking into account the two sources of information employed, data was obtained from 25 schools (52 percent) and 36 accredited programs (42 percent). In total, 36 syllabi were obtained for the analysis, 24 from schools and 12 from programs. Of these 36 syllabi analyzed, 21 were taught in 2011, 12 in 2012, and three in 2013. A total of four courses were exclusively online in nature.

Process of gathering information
Of the seven schools (S) and 21 programs (P) that did not offer a specific course on this subject, five of the schools and 12 of the programs stated that either ethical aspects were taught in a cross-cutting manner or woven into other courses in different subjects or other courses on ethical aspects were offered that, while not specifically focused on public health ethics, were related to this field, bearing titles such as “Public Health Law,” “Ethics and Research,” “Professional Ethics and Law,” “Health Care Ethics,” or “Ethics and Global Health.” None of these syllabi was included in this study, because they were not focused on public health ethics and they covered different topics, such as clinical ethics or law.
It is worth mentioning the high degree of variability found in the syllabi analyzed in terms of the title of the course, presentation format, type of content included in the document (description, schedule, reading lists, class or institutional policies, evaluation methods, assignments, grading, etc.), and amount of detail provided on objectives, competencies addressed, or topics studied. Only 18 syllabi included information on the number of U.S. academic credits assigned to the course: 12 syllabi with three credits (five S, seven P); four with two credits (three S, one P); one with four credits (one S); and one with one credit (one S).
The list of topics obtained is outlined in Tables 1 and 2. In total, 75 different topics were identified. Table 1 contains the 38 topics identified in six or more syllabi, and Table 2 contains the 37 topics included in five or less. As shown, a number of the topics in Table 1 are grouped. This is due to the fact that, in the opinion of the researchers, while each was evaluated independently, they in fact constitute different variants or nuances of the same, much more general theme. For example, “allocation of resources; rationing; priorities setting,” “social determinants of health; social epidemiology; health disparities and inequalities,” “justice; social justice; theories of justice,” “health care: reform in the U.S.,” and “health care: right to access” have been grouped together, given that they can be interpreted as different manners of approaching a general problem that might be labeled “justice and health.” All syllabi include required or recommended reading lists (articles, books, or chapters of books) for each of the lessons of the course. The size of the reading lists proved quite substantial in a number of cases.
Discussion
One of the first important points to emerge from this study was the large number of accredited schools and programs that state that they do not offer a specific course on PHE. While the majority might claim that the subject is taught in a cross-cutting manner or through other types of courses on ethics, the impression given is that the discipline is not afforded the importance—in view of the points established in the 2002 IOM report—it deserves. In 2006, in their research, Agee and Gimberl had already detected the scarcity of formal educational offers relating to ethics and law in accredited schools and public health programs, defining the situation as “disheartening” (Agee and Gimberl 2009). The reasons for this apparent lack of progress should be analyzed elsewhere.
A second important finding is that the topics more frequently included in the syllabi can be gathered and organized around eleven main topics (Table 1), supplemented by secondary topics (Table 2). On the basis of the information presented in Table 1, the eleven core topics could be summarized as follows: (1) the foundations of PHE; (2) autonomy and its limits; (3) infectious disease control; (4) justice and health; (5) research ethics; (6) health education and promotion: lifestyles and addictions; (7) environmental and occupational health; (8) screening; (9) genetics; (10) privacy and confidentiality; and (11) community-based practice and vulnerable populations. Obviously, the approach, specific content, and scope of each of these topics can vary significantly depending on the main focus of the course: ethical, legal, philosophical, sociological, political, clinical, hygienistic, and so on. It is also important to point out that these topics are merely headings employed for the purposes of simplifying and summarizing, grouping together contents that, while converging, are diverse in their more specific approaches.
The majority of these eleven topics can be found in the aforementioned reference articles, book texts, and documents that PHE has generated over the course of time. So it might be that the influence that these texts could have exercised on the training of the academics who currently teach the courses analyzed led them to include these topics more frequently. For example, most of the main topics appear in the most popular textbook within the courses, that of Bayer et al. (2007). The same might be said of one of the most recent textbooks, published by Dawson (2011). This text also is important because its main contributors are European, principally from the United Kingdom. This suggests that a certain degree of consensus might exist in relation to the importance of these 11 topics that reaches beyond the reality of the United States. But the weight given to each topic can be very different in each country. For example, Kessel found that the main topics in the postgraduate courses on PHE in the United Kingdom were related to moral and ethical theory, including the four principles approach, codes of ethics and professional ethics, and the topics of rationing and research ethics (Kessel 2003).
However, it goes without saying that “description” and “prescription” are by no means the same. That is, the fact that these 11 general topics are those that are most frequently included in U.S. courses, books, and documents on PHE does not necessarily imply that they should constitute the core material in this area. However, such considerations require more detailed and more profound discussion that falls beyond the scope of this paper. Moreover, perhaps such discussion should not be focused exclusively on the perspective from the United States but rather should take an international approach, from the point of view of global health. Nevertheless, a few remarks may be made. For example, a number of elements that appear in the lower section of the list of 11 topics, indicating that they are not as frequently included in courses—such as those relating to “privacy and confidentiality”—should undoubtedly be afforded greater importance in the future. Indeed, today, the problem of public health access to personal health information and, therefore, of the balance between privacy interests and potential public health benefits is recognized as a key topic within the future of PHE (Rothstein 2012). Secondly, deeper analysis of the detected content may lead to the conclusion that a number of topics currently included in courses less frequently (such as those appearing in Table 2) should be afforded greater importance in the future. In any event, creating international or regional spaces for the discussion of the core content of PHE in order to create a standardized core curriculum does appear advisable.
However, setting the key topics for the PHE courses does not prove sufficient. A study published in 2009, in which 45 semi-structured interviews with public health practitioners at 13 health departments in Michigan were analyzed, identified five broad categories of ethical issues (Baum et al. 2009). These categories were as follows: (a) determining appropriate use of public health authority; (b) making decisions relating to resource allocation; (c) negotiating political interference in public health practice; (d) ensuring standards of quality of care; and (e) questioning the role or scope of public health. This shows that the needs are not only theoretical but also practical. So it is necessary to prepare professionals both for ethical reflection and for ethical practice in the face of real problems. This requires a strong modification of the content of courses and deep changes within their methodological approach. Obviously this point is important for U.S. schools and programs on PH and for other regions of the world as well.
This work has various limitations that need to be taken into account. First, it should be pointed out that the rate of obtaining information, while of importance, may not be significant. A second significant limitation stems from the process of identifying the relevant topics. In spite of the consensus methodology used, the definition of what is a “topic” and what is not could be slightly different for other researchers. In many cases, the topics are intimately related to each other, and in some cases it has not been easy to separate and distinguish them. In general, when it came to drawing up the list of topics, the tendency was to be more open and inclusive than reductionist and exclusive. A sharper questioning linked with this limit could be done. Kessel thinks that PHE should be developed more in terms of analytical tools than in terms of a list of topics, although he also uses this latter approach in his paper (Kessel 2003). But both approaches are compatible and required. Needless to say that PHE aspires to give students knowledge, tools, and skills to deal with the daily ethical problems they will have to confront in their daily practice. But PHE courses also should train students to make actual use of these elements within the more morally troubled PH topics. In brief, both approaches need to define topics to be included in the syllabus of a course on PHE. A third limitation concerns the object of study itself (syllabi). The analysis of the documents is undoubtedly a relevant source of information. However, the actual teaching may, in practice, introduce many changes in the content within the learning processes. It is therefore difficult to ascertain with certainty, on the basis of the source of information used, whether or not the students who attend these courses are, in effect, being trained in these topics or in others. Moreover, learning objectives, educational strategies, and deliberation methods—three key points within ethical training—are not considered in our study. Thus, the results obtained in this paper are to be used with caution when it comes to attempting to determine the content actually taught in the courses on PHE in U.S. schools and programs. Further research is needed, employing different methodologies, before it is possible to generalize these results.
Conclusion
The introduction of PHE courses in the curricula of public health professionals is an evolving process in many regions of the world. The situation in the different countries of Europe is diverse, with huge differences between them, but it is at the very beginning. The state of practice in other regions or countries of the world, such as South America, Asia, or Australia, is not well known, and there is a lack of research on this topic. This is why this paper has focused on the United States, the country that has progressed most in this area in the last 25 years. But our results suggest that a lot of work remains to be done. Our methodology could be useful to increase our knowledge about the situation in other regions of the world, and it could be very interesting to replicate the study in different countries. To increase our knowledge about what we are now teaching about PHE all over the world might help us determine what we should teach from a global health ethics perspective in the future.
References
American Public Health Association. 2002. Principles of the ethical practice of public health. http://www.apha.org/NR/rdonlyres/1CED3CEA-287E-4185-9CBD-BD405FC60856/0/ethicsbrochure.pdf. Accessed July 5, 2014.
Aceijas, C., C. Brall, P. Schröder-Bäck, et al. 2012. Teaching ethics in schools of public health in the European region: Findings from a screening survey. Public Health Reviews 34(1): 1−7. http://www.publichealthreviews.eu/show/f/101. Accessed July 5, 2014.
Agee, B., and R.W. Gimberl. 2009. Assessing the legal and ethical preparedness of Master of Public Health graduates. American Journal of Public Health 99(8): 1505–1509. doi:10.2015/AJPH.2007.133173.
Baum, N.M., S.E. Gollust, S.D. Goold, and P.D. Jacobson. 2009. Ethical issues in public health practice in Michigan. American Journal of Public Health 99(2): 369–374.
Bayer, R., and A. Fairchild. 2004. The genesis of public health ethics. Bioethics 18(6): 473–492.
Bayer, R., and L.O. Gostin. 1990. Legal and ethical issues relating to AIDS. Bulletin of the Pan-American Health Organization 24(4): 454–468.
Bayer, R., L.O. Gostin, B. Jennings, and B. Steinbock. 2007. Public health ethics: Theory, policy, and practice. New York: Oxford University Press.
Beauchamp, D.E., and B. Steinbock, eds. 1999. New ethics for the public’s health. New York: Oxford University Press.
Bluestone, N.R. 1976. Teaching of ethics in schools of public health. American Journal of Public Health 66(5): 478–479.
Bradley, P., and A. Burls. 2000. Ethics in public and community health. New York: Routledge.
Callahan, D., and B. Jennings. 2002. Ethics and public health: Forging a strong relationship. American Journal of Public Health 92(2): 169–176.
Childress, J.F., R.R. Faden, R.D. Gaare, et al. 2002. Public health ethics: Mapping the terrain. Journal of Law, Medicine and Ethics 30(2): 170–178.
Cotter, L.E., J. Chevrier, W.N. El-Nachef, et al. 2009. Health and human rights education in U.S. schools of medicine and public health: Current status and future challenges. PLoS One 4(3): e4916. doi:10.1371/journal.pone.0004916.
Coughlin, S.S. 2000. Ethics in epidemiology at the end of the 20th century: Ethics, values, and mission statements. Epidemiologic Reviews 22(1): 169–175.
Coughlin, S.S., and T.L. Beauchamp, eds. 1996. Ethics and epidemiology. New York: Oxford University Press.
Coughlin, S.S., W.H. Katz, and D.R. Mattison. 1999. Ethics instruction at schools of public health in the United States. American Journal of Public Health 89(5): 768–770.
Council on Education for Public Health. 2012. Schools of public health and public health programs accredited. http://www.ceph.org/assets/Master_List.pdf. Accessed July 5, 2014.
Dawson, A., ed. 2011. Public health ethics. Cambridge, UK: Cambridge University Press.
Gebbie, K., L. Rosenstock, and L.M. Hernandez, eds. 2003. Who will keep the public healthy? Educating public health professionals for the 21st Century. Washington, DC: The National Academies Press.
Goodman, K., and R. Prineas. 1996. Towards an ethics curriculum in epidemiology. In Ethics and epidemiology, edited by S.S. Coughlin and T.L. Beauchamp, 290–303. New York: Oxford University Press.
Gostin, L.O. 2000. Public health law: Power, duty, restraint. Berkeley and New York: University of California Press and Milbank Memorial Fund.
Gostin, L.O. 2001. Public health, ethics, and human rights: A tribute to the late Jonathan Mann. Journal of Law, Medicine and Ethics 29(2): 121–130.
Gostin, L.O., ed. 2002. Public health law and ethics: A reader. Berkeley and New York: University of California Press and Milbank Memorial Fund.
Jennings, B., J. Kahn, A. Mastroianni, and L.S. Parker, eds. 2003. Ethics and public health: Model curriculum. https://repository.library.georgetown.edu/bitstream/handle/10822/556779/se0583.pdf?sequence=1. Accessed July 5, 2014.
Kass, N.E. 2001. An ethics framework for public health. American Journal of Public Health 91(11): 1776–1782.
Kessel, A.S. 2003. Public health ethics: Teaching survey and critical review. Social Science and Medicine 56(7): 1439–1445.
Lee, L.M., B. Wright, and S. Semaan. 2013. Expected ethical competencies of public health professionals and graduate curricula in accredited schools of public health in North America. American Journal of Public Health 103(5): 938–942. doi:10.2105/AJPH.2012.300680.
Mann, J.M. 1997. Medicine and public health, ethics and human rights. The Hastings Center Report 27(3): 6–13.
ASPHER and EUPHA. 2012. Working group on ethics and values in public health policy and practice in the European region: Developing a recommended curriculum on public health ethics. http://www.eupha.org/repository/sections/eph/Curriculum_in_PH_ethics_Report_of_ASPHER_Ethics_WG_31_Jan_2012.pdf. Accessed July 5, 2014.
Rothman, D. 1991. Strangers at the bedside: A history of how law and bioethics transformed medical decision-making. New York: Basic Books.
Rothstein, M.A. 2012. The future of public health ethics. American Journal of Public Health 102(1): 9.
Thomas, J.C. 2004. Skills for the ethical practice of public health. http://phls.org/CMSuploads/Skills-for-the-Ethical-Practice-of-Public-Health-68547.pdf. Accessed July 5, 2014.
Thomas, J.C., M. Sage, J. Dillenberg, and V.J. Guillory. 2002. A code of ethics for public health. American Journal of Public Health 92(7): 1057–1059.
University of Miami Ethics Programs. n.d. Epidemiology and public health ethics syllabi project. http://www.miami.edu/index.php/ethics/projects/EPHES. Accessed July 5, 2014.
Acknowledgments
The authors wish to thank, first and foremost, all the individuals from the various schools and programs who collaborated in this research and selflessly provided valuable information. Thanks also are afforded to Kenneth W. Goodman (University of Miami Ethics Program) for sharing information on PHE syllabi. Ronald Bayer (Mailman School of Public Health, University of Columbia, New York) supported this work from the outset, and Gavin McCune (Ofilingua, Granada) gave professional language assistance. This work was possible by virtue of the grant awarded by the Europubhealth Consortium (http://www.europubhealth.org ) to PSL for an academic stay as a visiting scholar at the Mailman School of Public Health of the University of Columbia in October and November 2012.
Conflicts of Interest
None declared.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Simón-Lorda, P., Barrio-Cantalejo, I.M. & Peinado-Gorlat, P. Content of Public Health Ethics Postgraduate Courses in the United States. Bioethical Inquiry 12, 409–417 (2015). https://doi.org/10.1007/s11673-015-9608-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11673-015-9608-x