The Effectiveness of Repetitive Transcranial Magnetic Stimulation for Post-stroke Dysphagia: A Systematic Review and Meta-Analysis
 Xin Wen
Xin Wen Zicai Liu
Zicai Liu Lida Zhong1
Lida Zhong1  Yang Peng
Yang Peng- 1Department of Rehabilitation Medicine, Yue Bei People's Hospital, Shaoguan, China
- 2School of Rehabilitation Medicine Gannan Medical University, Ganzhou, China
- 3Yue Bei People's Hospital, Shaoguan, China
Background: Repetitive transcranial magnetic stimulation (rTMS) applied to the mylohyoid cortical region has positive clinical effects on post-stroke. Therefore, we conducted a meta-analysis to investigate the efficacy of rTMS for patients with post-stroke dysphagia.
Methods: According to PRISMA guidelines, we searched the databases of MEDLINE (PubMed), Cochrane Library, Embase, Web of Science, CNKI, Wangfang. We searched for studies of randomized controlled trials (RCTs) of rTMS to treat dysphagia after stroke and screened by inclusion and exclusion criteria. Features of RCTs were extracted. The heterogeneity of the trials was measured by I2 statistic.
Results: In total, 11 RCTs with 463 dysphagia patients fulfilled our inclusion criteria. In our analysis, rTMS demonstrated a great beneficial effect for post-stroke dysphagia when combined with traditional swallowing exercises. Moreover, a greatly significant difference (P = 0.008) was noted based on stimulation frequency (high frequency vs. low frequency). Additionally, no significant difference (P = 0.53) was observed based on stimulation site (affected vs. unaffected hemisphere).
Conclusions: Overall, rTMS can effectively accelerate the improvement of swallowing function in patients with post-stroke swallowing disorders.
Introduction
Stroke, also known as a cerebrovascular accident, is a common cardiovascular disease with a high prevalence of morbidity, handicap, and fatality worldwide (GBD 2016 Stroke Collaborators, 2019). Deglutition disorders are one of the most widespread post-stroke complications. A previous study (Nepal and Sherpa, 2019) has shown that the prevalence of dysphagia in stroke survivors is up to 37–78%. The prevalence of post-stroke dysphagia reported from different studies also varies, and the prevalence varies by region. Furthermore, an estimated 41% of stroke patients in the United States experience difficulty swallowing (Crary et al., 2013), and nearly 51.14% of stroke inpatients have deglutition disorder in China (Zhang et al., 2021). Post-stroke dysphagia is an impaired swallowing function caused by an imbalance in the coordination of swallowing muscles and neural regulation, which prevents the patients from eating normally (Sandoval-Munoz and Haidar, 2021). Dysphagia is mainly manifested as salivation, coughing from drinking water, and prolonged eating times (Wilkinson et al., 2021). Therefore, patients with swallowing disorders often suffer from complications such as malnutrition, electrolyte disorders, aspiration, aspiration pneumonia, etc (Martino et al., 2005; Shigematsu and Fujishima, 2015). This seriously affects patients' health and quality of life, increases the burden on families and society, and even endangers patients' life safety (Arnold et al., 2016).
The routine treatment measures for swallowing disorders include the following: dietary modification (Reyes-Torres et al., 2019), postural substitution (Terré and Mearin, 2012), physical therapy (Kilinç et al., 2020; Liaw et al., 2020; Lin et al., 2021), acupuncture (Chen and Guo, 2018; Yuan et al., 2019), and sensorimotor stimulation (Simonelli et al., 2019; Wang et al., 2019; Oh et al., 2020). These treatments aim at improving the swallowing function and increasing the speed of eating, but their therapeutic effect is limited to some extent. Although a significant percentage of patients spontaneously regained the ability to swallow in a short period, more than 10% of patients still have residual swallowing problems after routine therapy (Smithard et al., 1997). Therefore, it is particularly important to boost the improvement of swallowing function more effectively in the early phases of stroke and reduce the risk of complications for the recovery of patients.
Hamdy et al. (1998) proposed that the rehabilitation of dysphagia after unilateral stroke was accompanied by an increased excitability of the unaffected hemisphere cortex. In recent years, repetitive transcranial magnetic stimulation (rTMS) has emerged as a treatment modality to enhance swallowing function by modulating cortical excitability (Jefferson et al., 2009; Khedr et al., 2009; Khedr and Abo-Elfetoh, 2010; Wang et al., 2017). It is acknowledged that low-frequency (1 Hz) rTMS has a suppressive effect on the cerebral cortex (Kobayashi et al., 2004; Mansur et al., 2005; Fregni et al., 2006), whereas high-frequency (≥1 Hz) rTMS has an excitatory effect on the cerebral cortex (Pascual-Leone et al., 1998; Peinemann et al., 2004). Lately, several studies (Khedr et al., 2009; Khedr and Abo-Elfetoh, 2010; Park et al., 2017) have demonstrated that rTMS can facilitate the recovery of swallowing function after stroke. However, the effectiveness of rTMS for post-stroke dysphagia is not well-documented by evidence-based medicine. Thus, we here intended to perform a systematic review of the randomized-controlled trials (RCTs) assessing the efficacy of rTMS on post-stroke dysphagia to offer an evidence-based basis for clinical treatment.
Methods
Protocol and Registration
Our systematic review was designed and implemented based on the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) guideline (Page et al., 2021). The study has been registered with Prospero (CRD42021288484).
Retrieval Strategy
Associated studies were performed on the databases of Cochrane Library, Embase, MEDLINE (PubMed), CNKI, and Wangfang. We retrieved RCTs of the efficacy of rTMS on post-stroke dysphagia. We did not restrict the language in the search process. The search included the keywords “stroke,” “dysphagia,” “swallowing disorders,” “deglutition disorders,” and “repetitive transcranial magnetic stimulation.” We choose only to included RCTs. In addition, we also manually retrieved some extra trials, which were subject-related and included studies, which were in reviews or meta-analyses. Using Pubmed database as an example, the search strategy was as follows (Table 1).
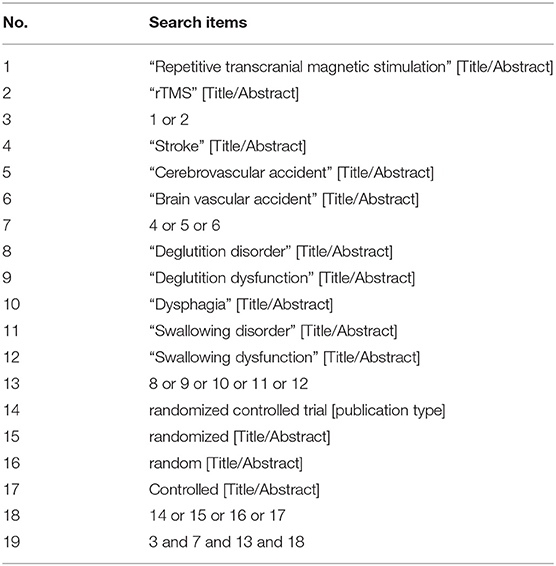
Table 1. The specific search strategy of Pubmed database.
Inclusion and Exclusion Criteria
Only studies with the following criteria were included: (1) the RCT trials with two or more arms, regardless of the sample size of each trial; (2) the peoples were diagnosed with post-stroke dysphagia through clinical examination; and (3) the same interventions were performed in the test and control groups, except that the test groups underwent rTMS. The exclusion criteria were as follows: (1) swallowing disorders are caused by other causes, such as Parkinson's disease, multiple sclerosis, cancer, et al.; (2) duplicated data; (3) inadequate data; and (4) the full text of the studies could not be obtained.
Study Selection Data Extraction
Firstly, all retrieved studies were imported into the document management system of EndnoteX20, and duplicated studies were deleted. Then, two researchers (WX and LZC) individually read the title and summary based on our inclusion and exclusion criteria. Afterward, we downloaded and read the full text of all studies which have been identified to be relevant and determined the eventually included trials after reading the full text. The inconsistencies during screening were settled through discussions, if necessary, together with another experienced reviewer (LHY).
Data Extraction and Quality Assessment
Two researchers (LZC and PY) individually extracted data from the included studies. The extraction included author, publication year, sample capacity, age, grouping, interventions, intervention time, measures, efficiency of the rTMS treatment, and so on. Any disagreements during the data collection were resolved by discussions. In addition, we contacted the corresponding author of the study to obtain the original data for the study when the data involved in a study were unclear or difficult to extract.
All included studies were evaluated for risk of bias, which had been done independently by two investigators (LZC and WJ) using the Cochrane risk of bias tool (Revman5.30). Risk bias assessment includes 7 dimensions: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting, and other bias. The discrepancies were resolved through intragroup discussions, if necessary, together with another experienced reviewer (LHY).
Statistical Analysis
All statistical analyses were conducted with Revman5.30. To evaluate heterogeneity, we utilized an I2-test. If I2 < 50%, the fixed-effect model was applied, otherwise, the random-effect model was adapted in the meta-analysis. Because trials did not assess patients using the same outcome indicators, we summarized data using changes pre-and post-intervention across groups. The effect size was expressed by a standardized mean difference (SMD) with a 95% confidence interval (CI).
Results
Research Result
Figure 1 depicts the process of study retrieval and selection. First, a total of 120 studies were identified from all databases, and after removing duplicates, 76 studies remained. Second, 40 studies were excluded after reading the title and summary, 6 were not available in full text, and then 19 were excluded after reading the full text. Eventually, 11 trials were included in our meta-analysis.
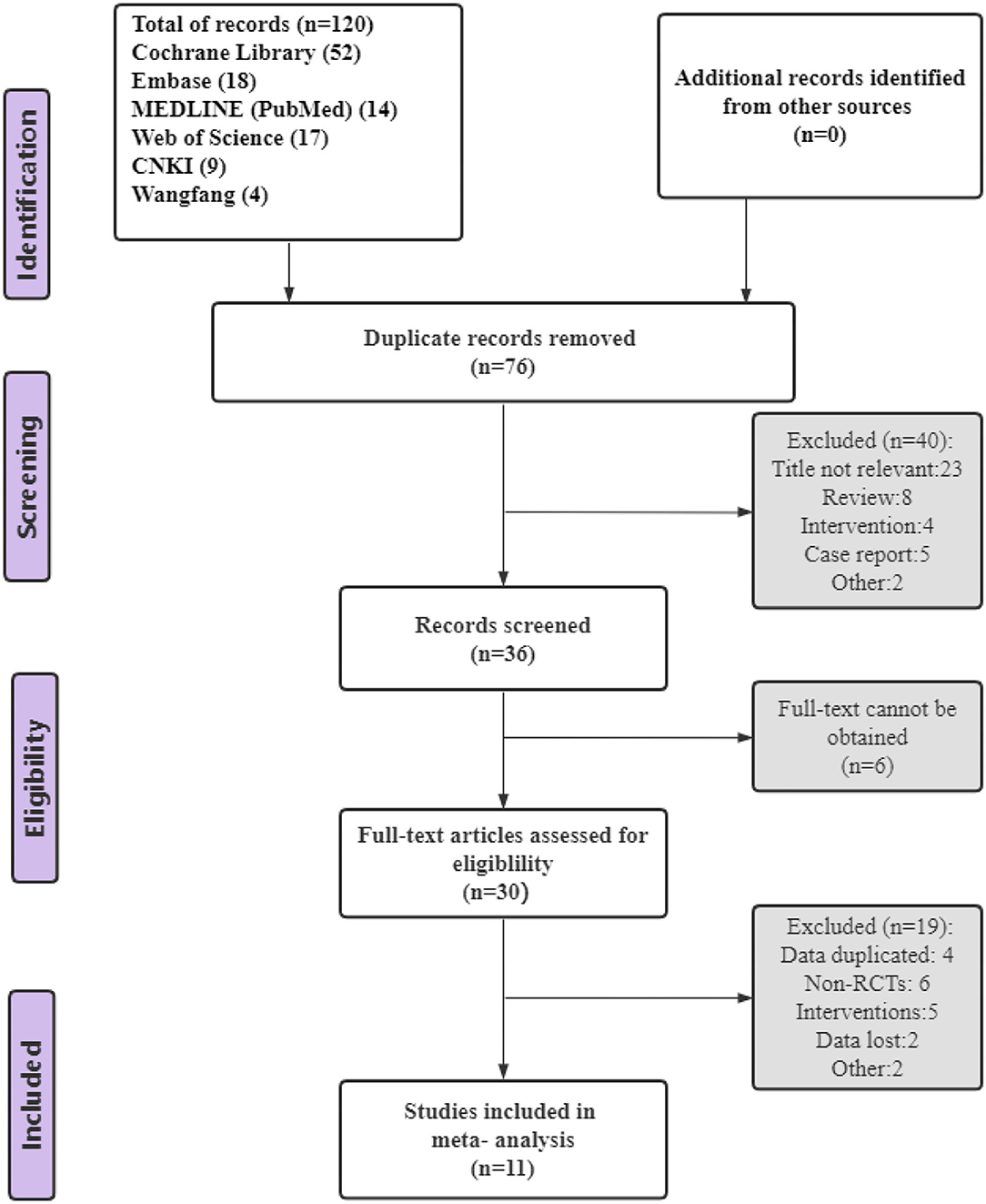
Figure 1. PRISMA flow chart of study selection.
Characteristics of the Trials
Table 2 presents the basic characteristics of the included trials, 11 RCTs with 463 patients, the sample size varied from 18 to 109 and the time after stroke was <6 months. Of these, 293 participants received rTMS and 170 participants only received conventional swallowing treatment. Table 3 shows the main parameters of rTMS, such as frequency, stimulation location, number of pulses, stimulation intensity, and stimulation time. In our meta-analysis, 6 studies (Khedr et al., 2009; Khedr and Abo-Elfetoh, 2010; Kim et al., 2011; Park et al., 2017; Cai et al., 2019; Zhong et al., 2021) used figure-eight coil, 3 studies (Ou-Yang et al., 2019; Zhang et al., 2020; Li et al., 2021) used circular coils, and 2 studies (Lim et al., 2014; Du et al., 2016) did not mention which coils were used.
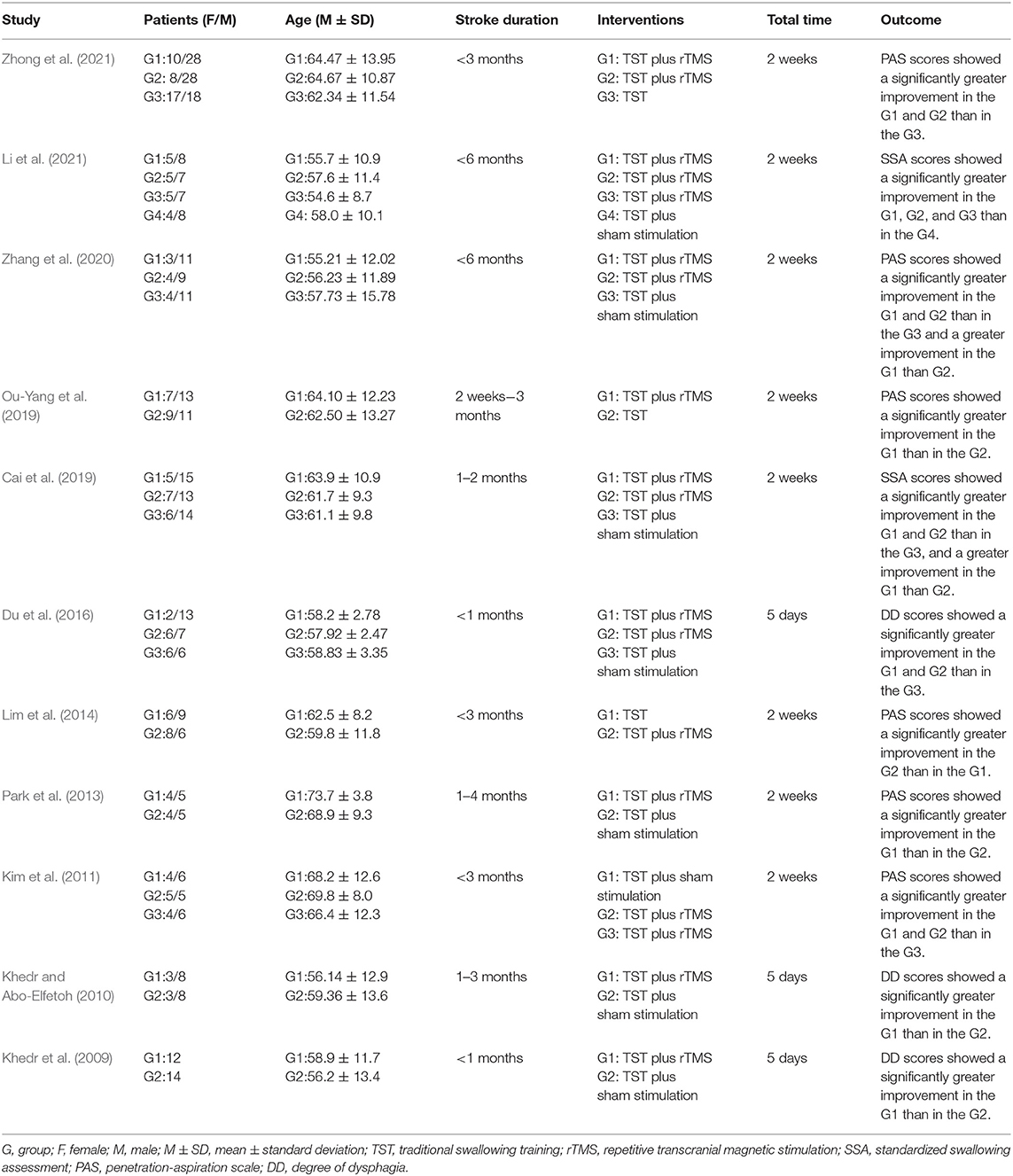
Table 2. The detailed features of the studies.
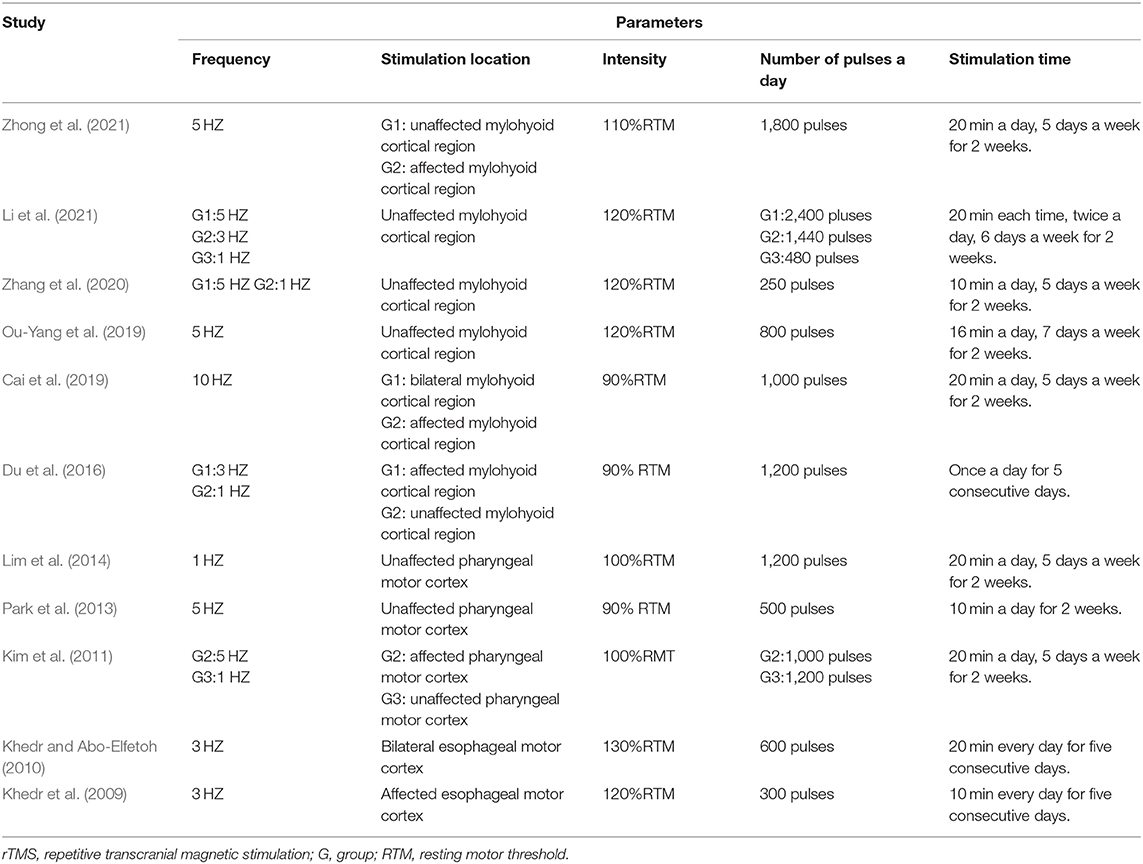
Table 3. Main parameters of rTMS.
Quality Assessment Result
Figures 2, 3 depict the risk bias assessment according to the Cochrane risk of bias tool (Revman5.30). The risk of selection bias and detection bias was unclear in most studies. However, in general, the risk of bias for the included studies was relatively low.
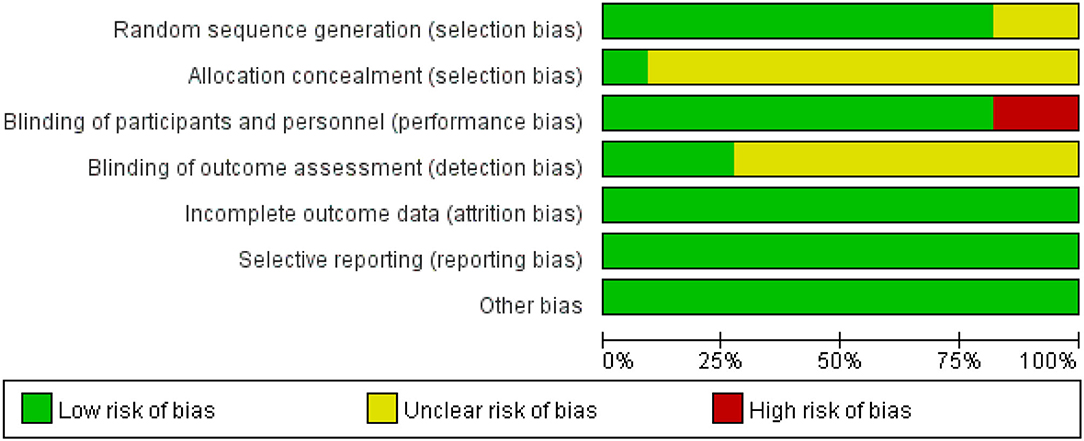
Figure 2. Risk of bias items shown as percentages across the included RCTs.

Figure 3. Risk of bias assessment for 11 RCTs.
Results of Statistical Analysis
In the meta-analysis of the 11 trials, statistically significant improvement was found in the experimental group compared with the control group (SMD = 2.15, 95 % CI = 1.61–2.70, I2 = 78 %; Figure 4). Of the 11 included studies, the control group in three studies performed only standard swallowing training, and the others performed sham stimulation in addition to standard swallowing training. The sham stimulation was the turning of the coils 180° instead of using a sham coil. The active stimulation had better therapeutic effects compared to either the conventional swallowing training or the sham stimulation, and a statistically significant difference was found between traditional swallowing training and placebo treatment. The stimulation of the affected or unaffected hemisphere and bilateral stimulation had better therapeutic effects compared to either the conventional swallowing training or the sham stimulation (SMD = 2.15, 95% CI = 1.61–2.69, I2 = 78%; Figure 5). However, no statistically significant difference was found between stimulating the affected hemisphere vs. the unaffected hemisphere vs. bilateral stimulation (I2 = 0%, p = 0.73; Figure 5). The subgroup analysis based on frequency revealed greatly significant improvement (SMD = 2.15, 95% CI = 1.61–2.70, I2 = 78%; Figure 6), and a statistically significant difference was found between the high-frequency group and low-frequency group (I2 = 85.7 %, p = 0.008; Figure 6). This analysis found that the effect size of 3 HZ was the largest (SMD = 2.28, 95% CI = 1.53–3.04, I2 = 34%; Figure 7) and the effect size of 1 HZ was the smallest (SMD = 1.26, 95% CI = 0.61–1.90, I2 = 45%; Figure 7), but there was no significant difference between the three groups of 1, 3, and 5 Hz (I2 = 56.9 %, p = 0.1; Figure 7).
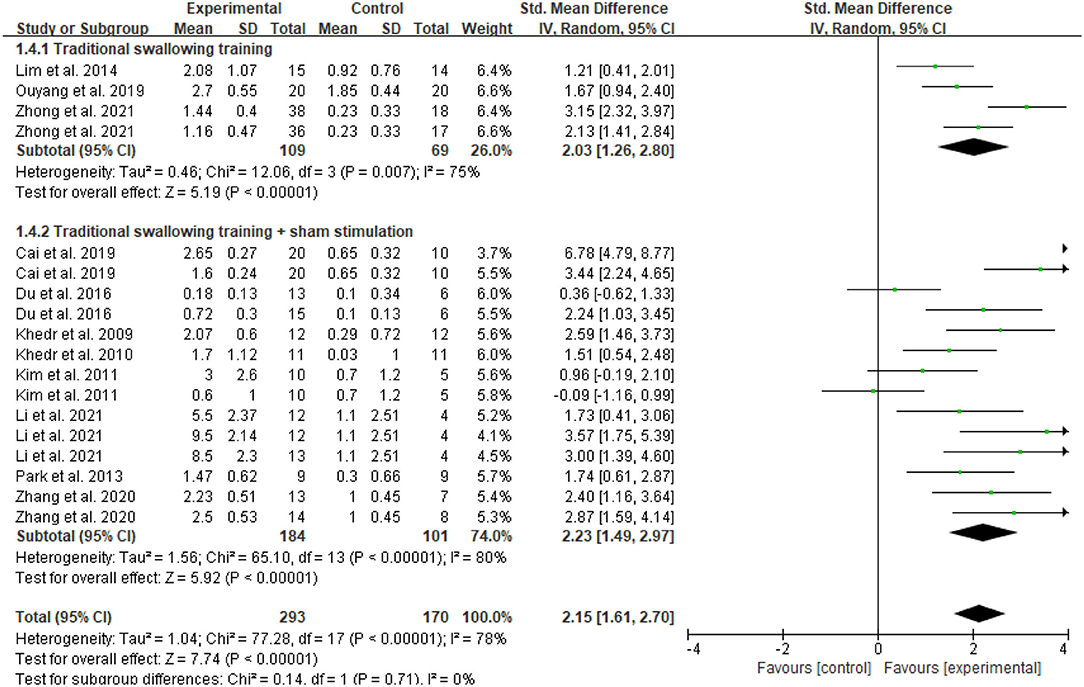
Figure 4. Forest plot of the overall effect analysis of rTMS.
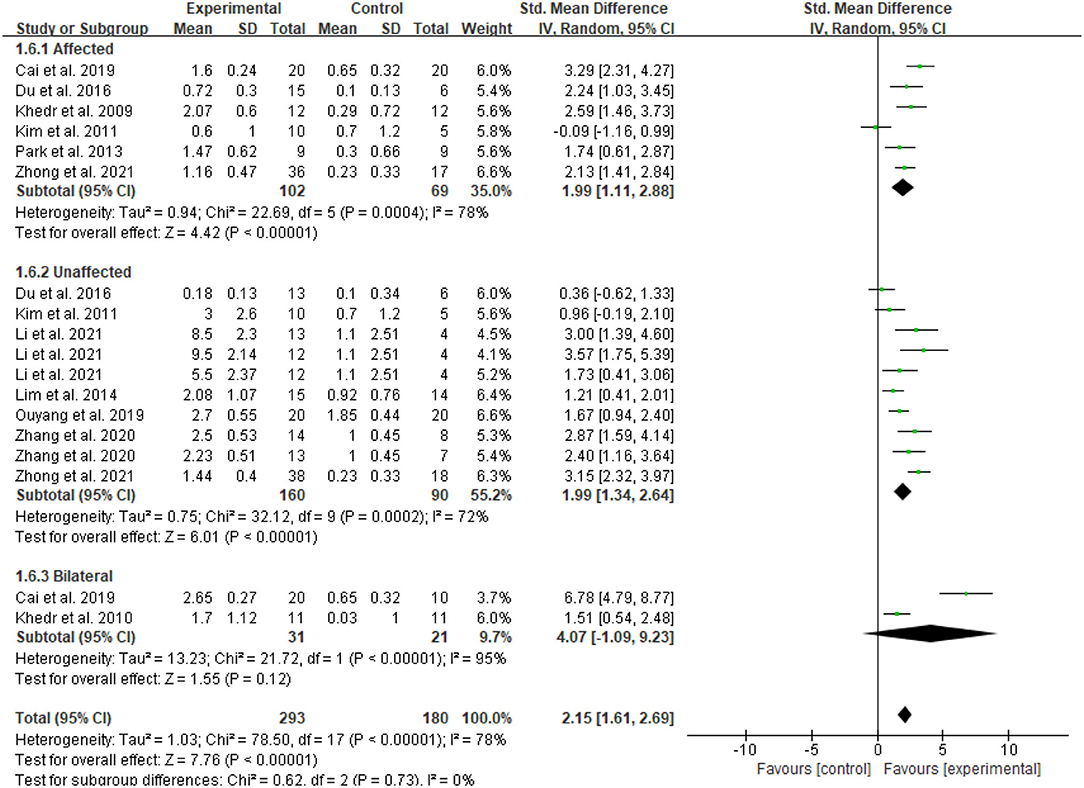
Figure 5. Forest plot for subgroup analysis according to the stimulation site.
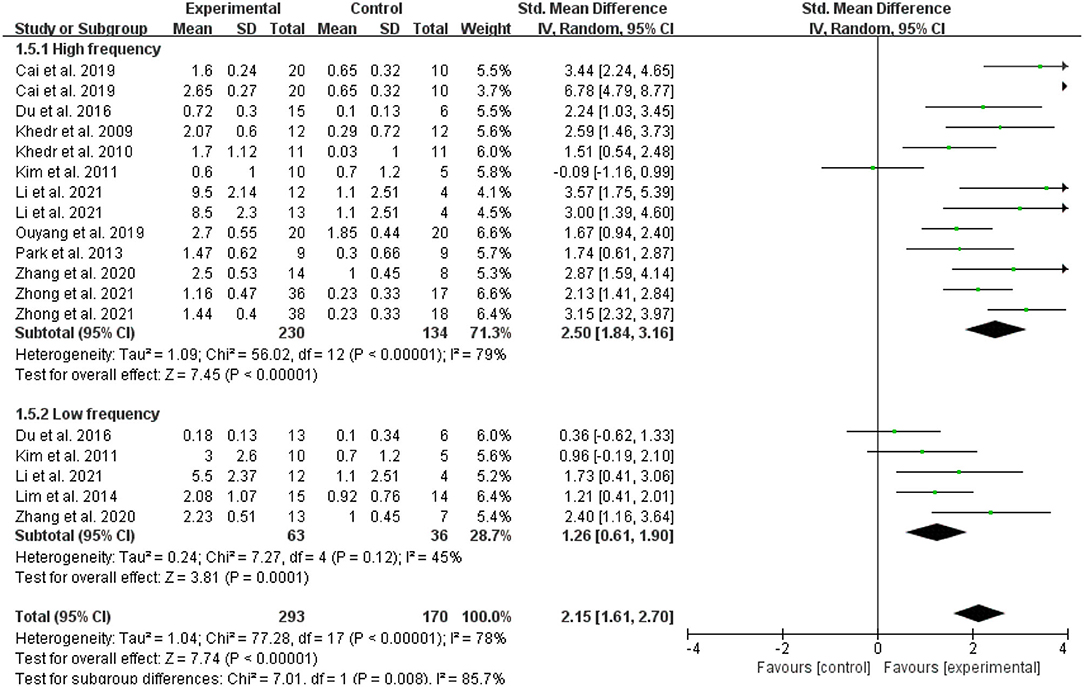
Figure 6. Forest plot for subgroup analysis according to stimulation frequency.
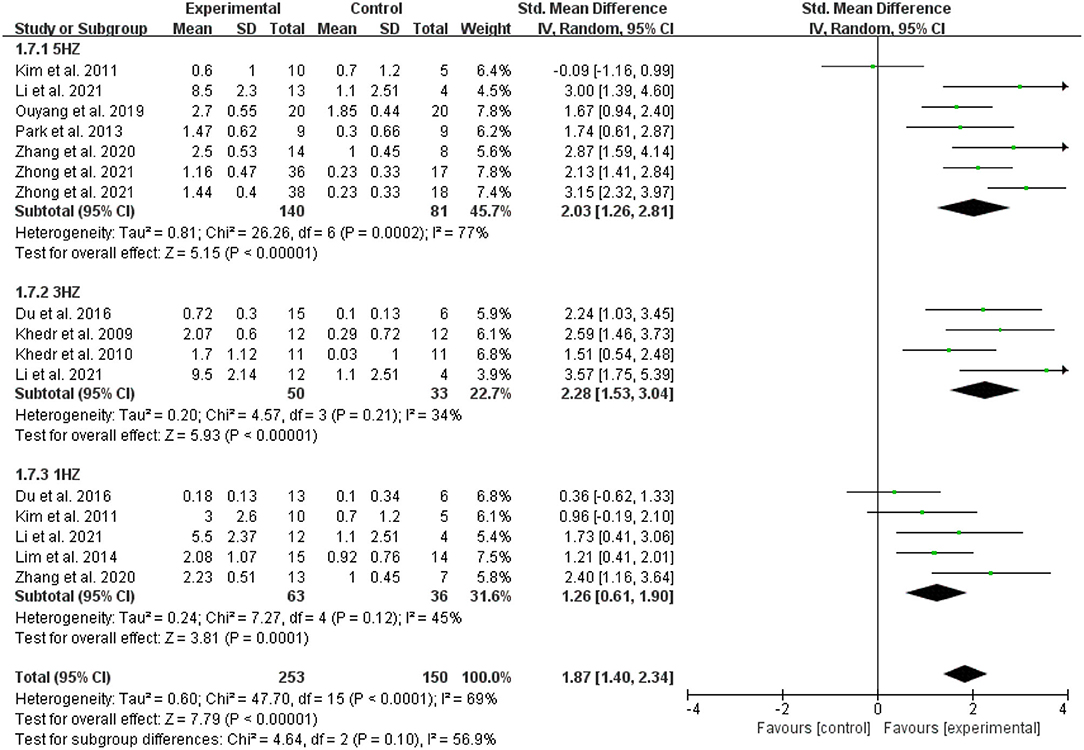
Figure 7. Comparison of the effect size of 5, 3, and 1 Hz.
Discussion
The results of this quantitative analysis showed that the overall effects of rTMS on the recovery of swallowing function were robust. This result was consistent with that of previous studies (Yang et al., 2015; Pisegna et al., 2016; Liao et al., 2017), which have reported that rTMS can efficiently contribute to the rehabilitation of swallowing function. Several studies have shown that both high-frequency and low-frequency stimulation can contribute to the improvement of swallowing function after stroke (Khedr et al., 2009; Verin and Leroi, 2009; Khedr and Abo-Elfetoh, 2010; Cheng et al., 2017b; Park et al., 2017; Ünlüer et al., 2019).
In addition, the result of subgroup analysis demonstrated greater effect sizes for stimulation of affected, unaffected, or bilateral hemisphere compared to standard swallowing training or placebo treatment. However, there were no significant differences between stimulating the affected hemisphere vs. the unaffected hemisphere vs. bilateral stimulation. A study by Zhong et al. (2021) proposed that 5 Hz-rTMS on either the unaffected or affected hemisphere improved post-stroke dysphagia, but there was no significant difference between the two. Cai et al. (2019) reported that bilateral stimulation is more efficient than unilateral stimulation in enhancing swallowing function after stroke. A case report (Momosaki et al., 2014) suggested bilateral stimulation could effectively facilitate the rehabilitation of post-stroke dysphagia. Similar results were reported by Park et al. (2013). However, a meta-analysis including the present RCTs gave not sufficient support that bilateral stimulation is more effective than unilateral. It has been shown that the pharyngeal cortical regions are presented in the bilateral cerebral hemispheres (Hamdy et al., 1996), it is now generally accepted that the swallowing functional areas in the cerebral cortex are found to have significant interhemispheric asymmetry (Wilmskoetter et al., 2018). Therefore, stimulation in either the healthy or the affected hemisphere improves swallowing function after stroke. Swallowing disorders occur when the “dominant” hemisphere is damaged and the unaffected non-dominant center is unable to compensate. Most patients with dysphagia may have damage to the dominant hemisphere of swallowing, and fewer relevant connections between the swallowing cortical networks of the damaged hemisphere may remain, so the recovery of swallowing function may be dependent on the unaffected side (Ou-Yang et al., 2019). Similarly, some researchers (Liao et al., 2017) also believed that stimulation on the unaffected hemisphere was superior to that on the affected hemisphere, but our study did not find this result. Khedr and Abo-Elfetoh (2010) and Cai et al. (2019) also thought that stimulation on the bilateral hemisphere was effective. In addition, a study on healthy volunteers by Sasegbon et al. (2021). found an inhibitory effect of high-frequency rTMS in the cerebellar vermis on pharyngeal motor cortical activity and swallowing behavior. Similarly, Zhong et al. (2021). showed that high-frequency rTMS applied to the cerebellum was effective in improving swallowing function in stroke patients. Furthermore, Lin et al. (2018) placed the coil of rTMS on the left postauricular mastoid in patients with brainstem injury to stimulate their vagus nerve, and found that the swallowing function of patients in the real stimulation group was significantly improved compared with the sham stimulation group. In conclusion, rTMS applied to the mylohyoid cortical region, pharyngeal motor cortex, esophageal motor cortex, cerebellum, and the left postauricular mastoid are all helpful in improving swallowing function. However, for the available studies, the cortical area of the mylohyoid muscle has been most frequently selected and has been noted to be effective. Gallas et al. (2007) thought that swallow recovery is associated with the cortical representation and mylohyoid pathways of swallowing muscle. Hamdy et al. (1996) found that mylohyoid EMG response amplitudes were larger than those of the pharyngeal response and esophageal response. We speculate that the amplitudes of the EMG response in the cortical region of the mylohyoid muscle are more obvious than others, and stimulation on the mylohyoid cortical region is also effective, so the mylohyoid cortical region is the most frequently stimulated site. Currently, there are many stimulation sites for dysphagia, and no studies have been conducted to compare its therapeutic efficacy, and the selection of the optimal stimulation site and its accurate localization are crucial to improve treatment for dysphagia. Therefore, future studies are required to investigate the effect of different stimulation sites on the therapeutic efficacy in order to find the optimal stimulation site and provide a basis for clinical treatment.
Furthermore, subgroup analyses based on frequency also revealed that high-frequency stimulation has a greater effect size than low-frequency stimulation. This result was similar to the previous review by Liao et al. (2017). Kim et al. (2011) thought that high-frequency rTMS on the affected hemisphere did not produce changes in swallowing function, while Khedr and Abo-Elfetoh (2010) and Cai et al. (2019) believed that high-frequency stimulation on the affected hemisphere had a significant benefit for post-stroke dysphagia. Ünlüer et al. (2019) found that 1 Hz rTMS promoted the recovery of swallowing function in the subacute period. It was usually believed that high frequency was typically used for the affected side increases cortical excitability, while the low frequency was typically used for the unaffected side decreases its excitability and equalizes cortical excitability in bilateral hemispheres, thus improving swallowing function. Hamdy et al. (2000) concluded that the recovery of post-stroke dysphagia depends on the functional compensation of the unaffected side, thus high-frequency stimulation on the unaffected hemisphere also could improve the swallowing function of patients. Unfortunately, all stroke patients involved in the included studies were in the acute or subacute period, and there were not enough RCTs for the chronic period. As a result, this meta-analysis can only analyze the effect of rTMS on the recovery of swallowing function in patients with acute or subacute stroke, but not on the recovery of swallowing function in patients with chronic stroke. A pilot study by Verin and Leroi (2009) suggested that 1 Hz rTMS improved swallowing function in stroke patients with a disease duration of more than 6 months, and since there was no sham and control group in this study, it could only show that low-frequency rTMS was beneficial for swallowing function recovery, but could not confirm that rTMS was more beneficial than the conventional swallowing training. Thus, they couldn't state whether rTMS was effective in improving swallowing function in patients with chronic post-stroke dysphagia. However, Cheng et al. (2017a) revealed that 5 Hz rTMS did not improve swallowing function compared to placebo treatment in chronic (>12 months) dysphagia. The reason why rTMS did not promote the recovery of swallowing function in patients in the chronic period may be that most selected participants with chronic post-stroke dysphagia have mild to moderate dysphagia, and there was little room for improvement in swallowing function, or it may be because the patients had extensive damage to the pharyngeal cortical areas of the bilateral cerebral hemispheres, and the effect was not significant regardless of the treatment measures. No studies have proven that there is an optimal intervention period during which rTMS is most effective, while beyond the optimal intervention period, rTMS is not effective. In addition, as rTMS is being used more frequently to treat post-stroke dysphagia, studies have begun to investigate whether different stimulation frequencies affect the treatment effect. Stimulation frequencies of 1, 3, and 5 Hz were used in the study. Considering the here included studies, 5 Hz is the most frequent and effective stimulation frequency. It was found that different stimulation frequencies would have different therapeutic effects as well. Therefore, to investigate the optimal stimulation frequency for rTMS, a subgroup analysis was performed. There was no significant difference in the effectiveness of 1, 3, and 5 Hz. However, a study by Li et al. (2021) also observed that the improvement of swallowing function after stroke was more obvious in 5 Hz rTMS compared to 3 Hz rTMS. Therefore, we could not determine which one is more effective, 5 Hz rTMS or 3Hz rTMS, and more studies can be done to directly compare the efficacy between them.
Fitzgerald et al. (2002) used 1 Hz rTMS of different stimulation intensities treatment on healthy volunteers, and found that the stimulation intensity of 115% resting motor threshold (RMT) was more effective than 85% RMT in inhibiting cortical excitability. A similar study was done by Mistry et al. (2007) they also used 1 Hz rTMS of different stimulation intensity treatments on patients with dysphagia and found that the stimulation intensity of 120% RMT was more effective than 80% RMT in improving the swallowing function of patients. Both studies were given low-frequency rTMS and compared the effects of different stimulation intensities on cortical excitability. There is no study regarding the effect of different stimulation intensities on cortical excitability with high-frequency rTMS, nor regarding the effect of the same stimulation intensity on the excitability with different stimulation locations. A study (Modugno et al., 2001) demonstrated that the greater the number of stimulus pulses, the wider the excitation of the cerebral cortex. Gilio et al. (2007) stimulated healthy subjects with different numbers of pulses of 5 Hz rTMS, and found that when the number of pulses was low, even when high-frequency stimulation was given, it did not excite the cerebral cortex, but rather inhibited it. It is generally believed that more pulses will have a more long-lasting benefit compared to fewer pulses, regardless of other stimulation factors. At present, there is no clinical study comparing rTMS with the different number of pulses for post-stroke dysphagia, nor is there a study comparing the effect of different stimulation times on the therapeutic effect, even though many articles do not explicitly state the stimulation time. A study by Khedr and Abo-Elfetoh (2010) found that rTMS plays an important role in the recovery of dysphagia in patients with lateral medullary syndrome and brainstem infarction. Otherwise, most studies have grouped patients with different stroke types for analysis, and no studies have investigated the effects of rTMS on patients with different stroke types. Therefore, future studies are required to investigate the effects of the different number of pulses and different stimulation times on the therapeutic efficacy, and to explore the effects of rTMS on patients with different stroke types.
Although we provided general information of currently available evidence for the application of rTMS in post-stroke dysphagia, our meta-analysis also had some limitations. First, TMS technology has some inherent limitations, for example, the localization of the stimulation site may not be very accurate, which has an impact on the treatment effect. The risk of seizures induced by TMS is about <0.03% (Rossi et al., 2021), and high-frequency TMS in the area of an acute or subacute stroke would increase the seizure risk. In addition, other limitations inherent to TMS technology include difficult delivery of a meaningful sham condition and high placebo response, inability to access non-cortical/deeper targets, lack of access to TMS at institutions, lack of portability, etc. Second, compared with the previous meta-analysis (Liao et al., 2017), more RCTs were included in this study, but the number of studies and patients included was relatively small. Third, different swallowing scales were used to assess the improvement of swallowing function, which may cause variations in the results. Finally, the heterogeneity across the included studies was relatively obvious, which may cause variations in the results. The reason for this high heterogeneity may be due to the different types of stroke patients, the different periods of stroke patients, and the different stimulation options of rTMS between studies.
Conclusion
Overall, rTMS can effectively promote the recovery of swallowing function in patients with post-stroke dysphagia. In our analysis, rTMS demonstrated a great beneficial effect for post-stroke dysphagia when combined with traditional swallowing exercises. Moreover, our findings suggested that high-frequency rTMS is more effective than low frequency. However, considering the high heterogeneity in this meta-analysis, we couldn't yet clear whether low-frequency stimulation is necessarily superior to high-frequency stimulation, and more RCTs need to be included for further analysis in the future. Additionally, no significant difference based on stimulation site (affected, unaffected and bilateral stimulation) was observed. In the future, more RCTs are needed to investigate the effect of different stimulation sites, different stimulation frequencies, different stimulation intensities, the different number of pulses, and different stimulation times on the therapeutic efficacy to find the optimal stimulation parameters and develop a personalized treatment plan for patients.
Data Availability Statement
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found in the article/supplementary material.
Author Contributions
HL: conceptualization, writing-reviewing and editing, data extraction, and assessing the risk of bias. XW: writing-original draft, study selection, research retrieval, and statistical analysis. ZL: study selection, data extraction, and writing-reviewing. LZ: article revision and writing-reviewing. YP: data extraction. JW: assessing the quality of studies. XG: article revision and grammar revision. All authors contributed to the article and approved the submitted version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Arnold, M., Liesirova, K., Broeg-Morvay, A., Meisterernst, J., Schlager, M., Mono, M. L., et al. (2016). Dysphagia in acute stroke: incidence, burden and impact on clinical outcome. PLoS ONE 11, e0148424. doi: 10.1371/journal.pone.0148424
Cai, Q., Yang, X., Sun, W., Xu, L., Liu, J., and Ma, M. (2019). Efficacy of bilateral high-frequency repetitive transcranial magnetic stimulation in the treatment of post-stroke dysphagia. Chin. J. Phys. Med. Rehabil. 41, 932–934. doi: 10.3760/cma.j.issn.0254-1424.2019.12.013
Chen, D., and Guo, H. (2018). [Therapeutic effects of acupuncture combined with rehabilitation training on dysphagia in post-stroke pseudobulbar palsy]. Zhongguo Zhen Jiu 38, 364–368. doi: 10.13703/j.0255-2930.2018.04.006
Cheng, I. K. Y., Chan, K. M. K., Wong, C. S., Li, L. S. W., Chiu, K. M. Y., Cheung, R. T. F., et al. (2017a). Neuronavigated high-frequency repetitive transcranial magnetic stimulation for chronic post-stroke dysphagia: a randomized controlled study. J. Rehabil. Med. 49, 475–481. doi: 10.2340/16501977-2235
Cheng, K. Y. I., Yiu, E., Wong, C. S., Li, L., Chiu, K., and Chan, K. (2017b). The use of 5 Hz rTMS to improve swallowing functions in chronic poststroke dysphagia. Dysphagia 32, 806–807. doi: 10.1007/s00455-017-9805-3
Crary, M. A., Carnaby, G. D., Sia, I., Khanna, A., and Waters, M. F. (2013). Spontaneous swallowing frequency has potential to identify dysphagia in acute stroke. Stroke 44, 3452–3457. doi: 10.1161/STROKEAHA.113.003048
Du, J., Yang, F., Liu, L., Hu, J., Cai, B., Liu, W., et al. (2016). Repetitive transcranial magnetic stimulation for rehabilitation of poststroke dysphagia: a randomized, double-blind clinical trial. Clin. Neurophysiol. 127, 1907–1913. doi: 10.1016/j.clinph.2015.11.045
Fitzgerald, P. B., Brown, T. L., Daskalakis, Z. J., Chen, R., and Kulkarni, J. (2002). Intensity-dependent effects of 1 Hz rTMS on human corticospinal excitability. Clin. Neurophysiol. 113, 1136–41. doi: 10.1016/S1388-2457(02)00145-1
Fregni, F., Boggio, P. S., Valle, A. C., Rocha, R. R., Duarte, J., Ferreira, M. J., et al. (2006). A sham-controlled trial of a 5-day course of repetitive transcranial magnetic stimulation of the unaffected hemisphere in stroke patients. Stroke 37, 2115–22. doi: 10.1161/01.STR.0000231390.58967.6b
Gallas, S., Moirot, P., Debono, G., Navarre, I., Denis, P., Marie, J. P., et al. (2007). Mylohyoid motor-evoked potentials relate to swallowing function after chronic stroke dysphagia. Neurogastroenterol. Motil. 19, 453–458. doi: 10.1111/j.1365-2982.2006.00892.x
GBD 2016 Stroke Collaborators (2019). Global, regional, and national burden of stroke, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol 18, 439–458. doi: 10.1016/S1474-4422(19)30034-1
Gilio, F., Conte, A., Vanacore, N., Frasca, V., Inghilleri, M., and Berardelli, A. (2007). Excitatory and inhibitory after-effects after repetitive magnetic transcranial stimulation (rTMS) in normal subjects. Exp. Brain Res. 176, 588–593. doi: 10.1007/s00221-006-0638-9
Hamdy, S., Aziz, Q., Rothwell, J. C., Power, M., Singh, K. D., Nicholson, D. A., et al. (1998). Recovery of swallowing after dysphagic stroke relates to functional reorganization in the intact motor cortex. Gastroenterology 115, 1104–1112. doi: 10.1016/S0016-5085(98)70081-2
Hamdy, S., Aziz, Q., Rothwell, J. C., Singh, K. D., Barlow, J., Hughes, D. G., et al. (1996). The cortical topography of human swallowing musculature in health and disease. Nat. Med. 2, 1217–1224. doi: 10.1038/nm1196-1217
Hamdy, S., Rothwell, J. C., Aziz, Q., and Thompson, D. G. (2000). Organization and reorganization of human swallowing motor cortex: implications for recovery after stroke. Clin. Sci. 99, 151–7. doi: 10.1042/CS19990300
Jefferson, S., Mistry, S., Michou, E., Singh, S., Rothwell, J. C., and Hamdy, S. (2009). Reversal of a virtual lesion in human pharyngeal motor cortex by high frequency contralesional brain stimulation. Gastroenterology 137, 841–849. 849.e1. doi: 10.1053/j.gastro.2009.04.056
Khedr, E. M., and Abo-Elfetoh, N. (2010). Therapeutic role of rTMS on recovery of dysphagia in patients with lateral medullary syndrome and brainstem infarction. J. Neurol. Neurosurg. Psychiatry 81, 495–9. doi: 10.1136/jnnp.2009.188482
Khedr, E. M., Abo-Elfetoh, N., and Rothwell, J. C. (2009). Treatment of post-stroke dysphagia with repetitive transcranial magnetic stimulation. Acta Neurol. Scand. 119, 155–61. doi: 10.1111/j.1600-0404.2008.01093.x
Kilinç, H. E., Arslan, S. S., Demir, N., and Karaduman, A. (2020). The effects of different exercise trainings on suprahyoid muscle activation, tongue pressure force and dysphagia limit in healthy subjects. Dysphagia 35, 717–724. doi: 10.1007/s00455-019-10079-w
Kim, L., Chun, M. H., Kim, B. R., and Lee, S. J. (2011). Effect of repetitive transcranial magnetic stimulation on patients with brain injury and Dysphagia. Ann. Rehabil. Med. 35, 765–771. doi: 10.5535/arm.2011.35.6.765
Kobayashi, M., Hutchinson, S., Théoret, H., Schlaug, G., and Pascual-Leone, A. (2004). Repetitive TMS of the motor cortex improves ipsilateral sequential simple finger movements. Neurology 62, 91–8. doi: 10.1212/WNL.62.1.91
Li, X., Guo, G., Li, Z., and Yan, Y. (2021). Effect of repetitive transcranial magnetic stimulation on swallowing function in patients with postoperative dysphagia with cranial defects after cerebral hemorrhage. Chin. J. Phys. Med. Rehabil. 43, 243–245. doi: 10.3760/cma.j.issn.0254-1424.2021.03.011
Liao, X., Xing, G., Guo, Z., Jin, Y., Tang, Q., and He, B. (2017). Repetitive transcranial magnetic stimulation as an alternative therapy for dysphagia after stroke: a systematic review and meta-analysis. Clin. Rehabil. 31, 289–298. doi: 10.1177/0269215516644771
Liaw, M. Y., Hsu, C. H., Leong, C. P., Liao, C. Y., Wang, L. Y., Lu, C. H., et al. (2020). Respiratory muscle training in stroke patients with respiratory muscle weakness, dysphagia, and dysarthria - a prospective randomized trial. Medicine 99, e19337. doi: 10.1097/MD.0000000000019337
Lim, K. B., Lee, H. J., Yoo, J., and Kwon, Y. G. (2014). Effect of low-frequency rTMS and NMES on subacute unilateral hemispheric stroke with dysphagia. Ann. Rehabil. Med. 38, 592–602. doi: 10.5535/arm.2014.38.5.592
Lin, C. H., Chung, S. Y., Lin, C. T., and Hwu, Y. J. (2021). Effect of tongue-to-palate resistance training on tongue strength in healthy adults. Auris Nasus Larynx 48, 116–123. doi: 10.1016/j.anl.2020.07.014
Lin, W. S., Chou, C. L., Chang, M. H., Chung, Y. M., Lin, F. G., and Tsai, P. Y. (2018). Vagus nerve magnetic modulation facilitates dysphagia recovery in patients with stroke involving the brainstem - a proof of concept study. Brain Stimul. 11, 264–270. doi: 10.1016/j.brs.2017.10.021
Mansur, C. G., Fregni, F., Boggio, P. S., Riberto, M., Gallucci-Neto, J., Santos, C. M., et al. (2005). A sham stimulation-controlled trial of rTMS of the unaffected hemisphere in stroke patients. Neurology 64, 1802–4. doi: 10.1212/01.WNL.0000161839.38079.92
Martino, R., Foley, N., Bhogal, S., Diamant, N., Speechley, M., and Teasell, R. (2005). Dysphagia after stroke: incidence, diagnosis, and pulmonary complications. Stroke 36, 2756–2763. doi: 10.1161/01.STR.0000190056.76543.eb
Mistry, S., Verin, E., Singh, S., Jefferson, S., Rothwell, J. C., Thompson, D. G., et al. (2007). Unilateral suppression of pharyngeal motor cortex to repetitive transcranial magnetic stimulation reveals functional asymmetry in the hemispheric projections to human swallowing. J. Physiol. 585, 525–538. doi: 10.1113/jphysiol.2007.144592
Modugno, N., Nakamura, Y., MacKinnon, C., Filipovic, S., Bestmann, S., Berardelli, A., et al. (2001). Motor cortex excitability following short trains of repetitive magnetic stimuli. Exp. Brain Res. 140, 453–459. doi: 10.1007/s002210100843
Momosaki, R., Abo, M., and Kakuda, W. (2014). Bilateral repetitive transcranial magnetic stimulation combined with intensive swallowing rehabilitation for chronic stroke Dysphagia: a case series study. Case Rep. Neurol. 6, 60–67. doi: 10.1159/000360936
Nepal, G. M., and Sherpa, M. D. (2019). Knowledge of dysphagia in stroke among nurses working in tertiary care hospital. Kathmandu Univ. Med. J. (KUMJ) 17, 126–130.
Oh, D. H., Park, J. S., Kim, H. J., Chang, M. Y., and Hwang, N. K. (2020). The effect of neuromuscular electrical stimulation with different electrode positions on swallowing in stroke patients with oropharyngeal dysphagia: A randomized trial. J. Back Musculoskelet. Rehabil. 33, 637–644. doi: 10.3233/BMR-181133
Ou-Yang, Y., Zhu, Q., Yan, W., Liu, X., Yi, W., Song, J., et al. (2019). Transcranial magnetic stimulation can relieve dysphagia after stroke. Chin. J. Phys. Med. Rehabil. 41, 261–265. doi: 10.3760/cma.j.issn.0254-1424.2019.04.005
Page, M. J., Moher, D., Bossuyt, P. M., Boutron, I., Hoffmann, T. C., Mulrow, C. D., et al. (2021). The PRISMA 2020 explanation and elaboration: updated guidance and exemplars for reporting systematic reviews. Bmj 372, n160. doi: 10.1136/bmj.n160
Park, E., Kim, M. S., Chang, W. H., Oh, S. M., Kim, Y. K., Lee, A., et al. (2013). Effects of bilateral repetitive transcranial magnetic stimulation on post-stroke dysphagia. Brain Stimul. 10, 75–82. doi: 10.1016/j.brs.2016.08.005
Park, J. W., Oh, J. C., Lee, J. W., Yeo, J. S., and Ryu, K. H. (2017). The effect of 5Hz high-frequency rTMS over contralesional pharyngeal motor cortex in post-stroke oropharyngeal dysphagia: a randomized controlled study. Neurogastroenterol. Motil. 25, 324–e250. doi: 10.1111/nmo.12063
Pascual-Leone, A., Tormos, J. M., Keenan, J., Tarazona, F., Cañete, C., and Catalá, M. D. (1998). Study and modulation of human cortical excitability with transcranial magnetic stimulation. J. Clin. Neurophysiol. 15, 333–43. doi: 10.1097/00004691-199807000-00005
Peinemann, A., Reimer, B., Löer, C., Quartarone, A., Münchau, A., Conrad, B., et al. (2004). Long-lasting increase in corticospinal excitability after 1800 pulses of subthreshold 5 Hz repetitive TMS to the primary motor cortex. Clin. Neurophysiol. 115, 1519–26. doi: 10.1016/j.clinph.2004.02.005
Pisegna, J. M., Kaneoka, A., Pearson, W. G. Jr, Kumar, S., and Langmore, S. E. (2016). Effects of non-invasive brain stimulation on post-stroke dysphagia: a systematic review and meta-analysis of randomized controlled trials. Clin. Neurophysiol. 127, 956–968. doi: 10.1016/j.clinph.2015.04.069
Reyes-Torres, C. A., Castillo-Martínez, L., Reyes-Guerrero, R., Ramos-Vázquez, A. G., Zavala-Solares, M., Cassis-Nosthas, L., et al. (2019). Design and implementation of modified-texture diet in older adults with oropharyngeal dysphagia: a randomized controlled trial. Eur. J. Clin. Nutr. 73, 989–996. doi: 10.1038/s41430-019-0389-x
Rossi, S., Antal, A., Bestmann, S., Bikson, M., Brewer, C., Brockmöller, J., et al. (2021). Safety and recommendations for TMS use in healthy subjects and patient populations, with updates on training, ethical and regulatory issues: expert guidelines. Clin. Neurophysiol. 132, 269–306. doi: 10.1016/j.clinph.2020.10.003
Sandoval-Munoz, C. P., and Haidar, Z. S. (2021). Neuro-Muscular Dentistry: the “diamond” concept of electro-stimulation potential for stomato-gnathic and oro-dental conditions. Head Face Med. 17, 2. doi: 10.1186/s13005-021-00257-3
Sasegbon, A., Niziolek, N., Zhang, M., Smith, C. J., Bath, P. M., Rothwell, J., et al. (2021). The effects of midline cerebellar rTMS on human pharyngeal cortical activity in the intact swallowing motor system. Cerebellum 20, 101–115. doi: 10.1007/s12311-020-01191-x
Shigematsu, T., and Fujishima, I. (2015). [Dysphagia and swallowing rehabilitation]. Brain Nerve 67, 169–182. doi: 10.11477/mf.1416200109
Simonelli, M., Ruoppolo, G., Iosa, M., Morone, G., Fusco, A., Grasso, M. G., et al. (2019). A stimulus for eating. the use of neuromuscular transcutaneous electrical stimulation in patients affected by severe dysphagia after subacute stroke: a pilot randomized controlled trial. NeuroRehabilitation 44, 103–110. doi: 10.3233/NRE-182526
Smithard, D. G., O'Neill, P. A., Martin, D. F., and England, R. (1997). Aspiration following stroke: is it related to the side of the stroke? Clin. Rehabil. 11, 73–6. doi: 10.1177/026921559701100111
Terré, R., and Mearin, F. (2012). Effectiveness of chin-down posture to prevent tracheal aspiration in dysphagia secondary to acquired brain injury. a videofluoroscopy study. Neurogastroenterol. Motil. 24, 414–9. e206. doi: 10.1111/j.1365-2982.2011.01869.x
Ünlüer, N., Temuçin, Ç., Demir, N., Serel Arslan, S. E. L. E. N., and Karaduman, A. (2019). Effects of low-frequency repetitive transcranial magnetic stimulation on swallowing function and quality of life of post-stroke patients. Dysphagia 34, 360–371. doi: 10.1007/s00455-018-09965-6
Verin, E., and Leroi, A. M. (2009). Poststroke dysphagia rehabilitation by repetitive transcranial magnetic stimulation: a noncontrolled pilot study. Dysphagia 24, 204–210. doi: 10.1007/s00455-008-9195-7
Wang, Z., Song, W. Q., and Wang, L. (2017). Application of noninvasive brain stimulation for post-stroke dysphagia rehabilitation. Kaohsiung J. Med. Sci. 33, 55–61. doi: 10.1016/j.kjms.2016.11.007
Wang, Z., Wu, L., Fang, Q., Shen, M., Zhang, L., and Liu, X. (2019). Effects of capsaicin on swallowing function in stroke patients with dysphagia: a randomized controlled trial. J. Stroke Cerebrovasc. Dis. 28, 1744–1751. doi: 10.1016/j.jstrokecerebrovasdis.2019.02.008
Wilkinson, J. M., Codipilly, D. C., and Wilfahrt, R. P. (2021). Dysphagia: evaluation and collaborative management. Am. Fam. Phys. 103, 97–106.
Wilmskoetter, J., Martin-Harris, B., Pearson, W. G. Jr, Bonilha, L., Elm, J. J., Horn, J., et al. (2018). Differences in swallow physiology in patients with left and right hemispheric strokes. Physiol. Behav. 194, 144–152. doi: 10.1016/j.physbeh.2018.05.010
Yang, S. N., Pyun, S. B., Kim, H. J., Ahn, H. S., and Rhyu, B. J. (2015). Effectiveness of non-invasive brain stimulation in dysphagia subsequent to stroke: a systemic review and meta-analysis. Dysphagia 30, 383–91. doi: 10.1007/s00455-015-9619-0
Yuan, Y., Cai, X. H., Chen, F., Chen, D. X., Gao, Y., Liu, Z. Z., et al. (2019). [Clinical trials of acupuncture treatment of post-stroke dysphagia by deep acupuncture of Tiantu (CV22) in combination with swallowing rehabilitation training]. Zhen Ci Yan Jiu 44, 47–50. doi: 10.13702/j.1000-0607.170788
Zhang, M., Li, C., Zhang, F., Han, X., Yang, Q., Lin, T., et al. (2021). Prevalence of dysphagia in China: an epidemiological survey of 5943 participants. Dysphagia 36, 339–350. doi: 10.1007/s00455-020-10138-7
Zhang, Y., Wang, Q., Meng, P., Yang, M., Li, Z., Zhang, Z., et al. (2020). The effects of different frequencies repetitive transcranial magentic stimulation on post-stroke dysphagia. Chin. J. Phys. Med. Rehabil. 42, 295–299. doi: 10.3760/cma.j.issn.0254-1424.2020.04.002
Keywords: stroke, dysphagia, repetitive transcranial magnetic stimulation, meta-analysis, effectiveness
Citation: Wen X, Liu Z, Zhong L, Peng Y, Wang J, Liu H and Gong X (2022) The Effectiveness of Repetitive Transcranial Magnetic Stimulation for Post-stroke Dysphagia: A Systematic Review and Meta-Analysis. Front. Hum. Neurosci. 16:841781. doi: 10.3389/fnhum.2022.841781
Received: 22 December 2021; Accepted: 17 February 2022;
Published: 17 March 2022.
Edited by:
Anna-Sophia Wahl, University of Zurich, SwitzerlandReviewed by:
Marcello Romano, Azienda Ospedaliera Ospedali Riuniti Villa Sofia Cervello, ItalyJessica Frey, University of Florida, United States
Copyright © 2022 Wen, Liu, Zhong, Peng, Wang, Liu and Gong. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Huiyu Liu, liuhuiyudoctor@sohu.com; Xiaoqian Gong, 13826380678@139.com
†These authors have contributed equally to this work and share first authorship