
Abstract
Although medical confidentiality is widely recognized as an essential principle in the therapeutic relationship, its systematic and coherent practice has been an ethically challenging duty upon healthcare providers due to various concerns of clinical, moral, religious, social, ethical and legal natures. Medical confidentiality can be breached to protect the patient and/or others if maintaining confidentiality causes serious harm. Healthcare professionals may encounter complicated situations whereby the divulgence of a patient’s confidential information may pose a threat to one party whereas the concealment of such information may cause harm to another. After deliberating on the Islamic concept of harm (ḍarar), this paper focuses on the dual duty and conflicts of interests faced by healthcare professionals in the practice of medical confidentiality. Referring to serious infectious diseases with a special mention of AIDS, this study also provides discourse on how healthcare professionals deal with difficult scenarios of conflicts of interests and ethical dilemmas.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Medical confidentiality implies that the physician acknowledges the patient’s need for confidentiality vis-à-vis the medical care he receives. This aspect of the doctor–patient relationship is about building trust and protecting the patient’s dignity (Siegler, 1995, p. 150). However, with time, the connotations around medical confidentiality have changed, and new issues and complications started to appear surrounding it. Codes of medical practice, such as the International Code of Medical Ethics of the World Medical Association (WMA), justify breaching confidentiality if disclosure is necessary due to risk of harm to the patient or others likely to be affected.
Beauchamp and Childress assert that “the obligations of medical confidentiality are not, at present, well-delineated and need restructuring” because this principle is observed to be compromised in several ways in everyday clinical practice (2001, p. 312). Based on recent studies, an increment has been noticed in these concerns surrounding medical confidentiality. In addition, to complicate the situation, “there is not a single statute or common body of laws governing confidentiality” (Herring, 2008, p. 193). Because of the uncertainty of doctors and their illogical decisions in divulging patient information, people have become victims in some cases.
Ethicists, law professionals, members of healthcare, and members of society at large are close to reaching a consensus about the rightfulness of confidentiality breaches to protect patients and others from serious harm. In other words, the protection of patients or others from serious harm is generally deemed as a justified warrant to breach confidentiality (General Medical Council, 2017, p. 13; The Nursing and Midwifery Council, 2002, Code 5; The Islamic Fiqh Academy, 1993). Physicians often encounter ethical dilemmas between maintaining patient confidentiality versus the disclosure of confidential information to fulfill their responsibility of protecting third parties or the general public from danger. A significant factor that can impinge on medical confidentiality is the disclosure of patient information to individuals or groups, such as the police, social workers, or companies dealing with occupational health. By and large, health professionals come across the problem of having to breach the medical confidentiality of individuals affected by psychiatric diseases, contagious diseases, venereal diseases, criminal or abusive cases, and genetic testing.
This case of dual loyalty, where the healthcare worker is obliged to care for the patient as well as to protect others, generates a conflict of interests. The contrasting duties of confidentiality and disclosure subsequently confuse health workers, as they are acutely uncertain, at times, about the legal and ethical positions in certain scenarios. The WMA’s International Code of Medical Ethics states, “It is ethical to disclose confidential information when a patient consents to it or there is a real and imminent threat of harm to the patient or others. This threat can be only removed by a breach of confidentiality” (2015, p. 53). The WMA clearly mentions that there are exceptions in maintaining confidentiality as some occasions “raise very difficult ethical issues of physicians” (Williams, 2015, p. 53).
Against this background, this paper first attempts to explain the concept of harm (ḍarar) and medical confidentiality from an Islamic jurisprudence (fiqh) perspective. It then deliberates on the vitality of the principle of harm elimination in the medical confidentiality practice followed by an analysis of dual duties related to medical confidentiality in general and particularly in cases related to serious infectious diseases.
Harm (Ḍarar) in Islamic Jurisprudence
Ḍarar can be defined as any kind of damage inflicted on a person—be it physical injury or financial loss, or mental trauma (Ibn Fāris, 1991, 3: 360). Like many Arabic terms, the word ḍarar embodies a cluster of implications related to diverse consequences resulting from detrimental actions (Al-Kufawī, 2010, p. 578). It can also be described as the denial of legal rights to someone and their deprivation of lawful and rightful benefits. Ḍarar is also explained as a defect that befalls a valuable property, human body or dignity (ʿAlī al-Khafīf, 2000, p. 38).
The earlier scholars defined ḍarar in various ways. Ibn al-‘Arabī (d. 1148 in Morocco, Mālikī) defined ḍarar as pain, leaving no similar or bigger benefit against it. Al-Rāzī (d. 1210 in Afghanistan, Shāfiʿī) viewed it as emotional distress and whatever leads to mental pain. Then, he explained that a benefit is a pleasure and its causes (1979, 2: 143). Al-Manāwī (d. 1621 in Cairo, Shāfiʿī) viewed ḍarar as a deliberate action to cause evil (mafsadah) upon another (1937, 6: 43). Mafsadah technically means the opposite of a benefit (maṣlaḥah), and figuratively, it implies the cause of harm. Abū Ḥāmid al-Ghazālī (d. 1111 in Iran, Shāfiʿī) elaborated on maṣlaḥah as “the attainment of benefits and the repulsion of harms” and postulated a comprehensive definition for it, “preservation of the five objectives of the Sharīʿah, i.e., preservation of religion, body, intellect, progeny and wealth” (1993, 1: 174). In addition, any act that breaches the principles of the Sharīʿah is considered mafsadah. Similar to maṣlaḥah, the gravity of mafsadah is also categorized according to the ḍarūriyyāt, ḥājiyyāt and taḥsīniyyāt, which are three categories of Maqāṣid al-Sharīʿah.
Maqāṣid al-Sharīʿah (higher objectives of Sharīʿah) are consensually perceived as the five universal legal purposes, namely the protection of religion, body, intellect, progeny, and wealth. Noticeably, all nations and communities have acknowledged the importance of these five foundational objectives. Ḍarūriyyāt refers to the necessary things for the protection of faith, life, intellect, family, and wealth. Their existence is crucial for the success of here and the hereafter, and their absence disrupts the life system and spreads corruption. Ḥājiyyāt refers to what facilitates human life on earth and removes troubles. Taḥsīniyyāt refers to what makes life disciplined and morally sound. Its absence neither affects the system of life nor causes significant troubles, but leaves the defect and imperfections of things. The gravity of harm is counted based on which category of Maqāṣid it inflicts.
Incorporating these various implications, contemporary scholar Aḥmad Mawāfī defined ḍarar as “the violation of the legitimate interests (maṣlaḥah mashrūʿah) of one’s own or of others by the infringement of rights, abuse of power or negligence” (Aḥmad Mawāfī, 1997, p. 97). This definition seems comprehensive and carries the major implications of ḍarar pinned down by erudite Islamic scholars.
Criteria of Ḍarar
Some kinds of harm are normal and they are part of life. Therefore, in Islamic jurisprudence, the jurists have identified certain conditions to determine actual and significant harm that are required to be eliminated. The major criteria for considering something as harm from an Islamic jurisprudence perspective are discussed below.
The Harm Should Be Real
The word "real" here refers to either harm that has happened or is highly probable to happen in the immediate future. However, if the harm is a distant possibility or is unlikely to happen or is just pure imagination, then it is excluded (Shubayr, 2007, p. 171). The Sharīʿah does not give weight to imaginations and rare incidents based on the maxim “no consideration is given to illusion” (lā ʿIbrata li al-Tawahhum). Some argue, for example, that a growing population is a threat to the economy of a country, so birth control has to be applied to overcome this problem. However, this argument was not given any heed by Sharīʿah scholars because of its weak basis and the unrealistic nature of the assumption. In addition, new resources and economical grounds are being regularly invented as a norm on earth since the beginning of human history. On one side, people are born and on the other, people die. At times, the death toll is huge, as it was in the instance of the pandemic. Nevertheless, selling grapes to the winemaker is prohibited according to the Islamic legal maxim, “harm must be averted as much as possible” because the possibility of using the grapes for winemaking in his case is high.
According to the dominant opinion in four sunnī schools, any enterprise which results in disruption of benefit is considered as a real harm. In addition, if the disruption is probable or anticipated (in between doubt and assurance), then Mālikī and Ḥanbalī scholars consider that action as harmful because predominant suppositions are considered certain things in fiqh (Ibn Mufliḥ, 2003, 4: 42). Moreover, the principle of "blocking means" (sadd adh-dharā’iʿ) is also in line with prohibiting pending harm. Sadd dharā’iʿ indicates that “blocking the means to an expected end which is likely to materialise if the means towards it is not obstructed. Blocking the means must necessarily be understood to imply blocking the means to evil, not to something good” (Kamali, 2003, p. 269). The principle of sadd dharā’iʿ centres on the concept of prevention of harm before it takes place. However, Shāfiʿī and Ḥanafī Schools do not always consider the probable harmful things as real harm because there is the possibility of non-occurrence of the assumed things, as a result, they issue only discouragement, not prohibition (Al-Kāsānī, 1986, 5: 223). For example, the rulings upon the selling of weapons to criminals are different according to various schools of law. In Shafiʿī School, though it is detestable (makrūh), the act/contract is considered valid selling. In the view of Ḥanafī School, the selling is valid, but if the seller knows the buyer is a real criminal, then it is of severe detestation (karāhat taḥrīmiyyah) and if otherwise, it is merely detestable. According to Ḥanbalī and Mālikī scholars, the mentioned selling is prohibited as well as invalid.
The Harm Should Be Excessive (Fāḥish)
The application of rules and maxims regarding eliminating harm is advanced only after distinguishing the serious harms from trivial ones. The size of harm could be weighed according to intensity, frequency, and duration. Since insignificant and minimal harm is largely tolerated and ignored in life, the rules and maxims of harm elimination are not applied therein. However, there is no single inclusive yardstick to determine whether harm is serious or not. Some jurists opine that the yardstick is whenever a person has a legitimate right to use something, then the consequence of that act is not excessive.
Shāfiʿī and Ḥanafī scholars attach more importance to the “right of ownership”, and therefore as long as a person utilizes his property, it is not considered harmful except on a few occasions (al-Ḥaṣkafī, 2002, 5: 448). They argue if otherwise, it culminates in restricting the freedom of a person in using his property. Right of ownership gives the owner the ability to do with the property whatever they choose. In contrast, Mālikī and Ḥanbalī scholars give weight to the maxim of “no harm” to “right of ownership”. Therefore, people are barred from the utilization of their owned property too in many cases, if their actions pose a danger to others (al-Tusūlī, 1998, 2: 335).
It can be argued that the second approach is more suitable because it combines the values of public welfare and is in line with the Islamic legal maxim “prevention of harm is preferred to the attainment of benefit.” It is to be noted that, based on the Islamic legal maxim “custom is authoritative,” the prevailing customs in a particular area are also considered a yardstick to measure whether harm is excessive or not. The prevailing custom has been the basis of many legal verdicts in Islamic history. Likewise, excessiveness of harm is determined by considering the frequency of occurrence; if harm takes place repeatedly, it is considered a significant harm and if otherwise, it is negligible. The excessiveness is not only measured in its material aspect but also in its moral aspect; like an assault on dignity in public.
The Infliction Should Occur as a Result of Infringement or Arbitrariness or Negligence
An action is called ḍarar if it happens due to infringement, arbitrariness or negligence without a legitimate reason or legal right. Infringement (taʿaddī) means the disruption of legitimate benefits without any right. This term is also used for doing prohibited things and invading others’ rights. Likewise, doing good things with a bad intention is also regarded as an infringement. In Sharīʿah, the intention is regarded as a key criterion to determine whether an act is punishable or pardonable, as well as to decide whether the punishment falls in the category of predetermined (ḥadd) or discretionary (taʿzīr) (Powers, 2006, p. 173). Likewise, one of the five universal Islamic maxims is “matters are judged by their objectives (intention)”. Therefore, an act is regarded as taʿaddī in three situations: (1) If the act is not held with a legal justification; (2) if it invades others’ rights; (3) or if the agent has an illegal objective in using his right.
Jurists of the four sunnī madhāhib have regarded transgression as a condition for holding someone liable for being causative of any harm. Mālikī scholar al-Shāṭibī (d. 1388 in Granada) explicates three elements that are regarded as signs of bad intention in one’s undertakings. They are (1) an act in which no benefit has been paid off in lieu except infliction, (2) an act that is recognized as the most probable place of harm in light of circumstantial evidence, and (3) negligence of social values that are approved by the Sharīʿah (al-Shāṭibī, 2004, pp. 359–361).
Arbitrariness (taʿassuf) means abusive use of rights. On various occasions, it is done by employing legal stratagems. Two features are largely seen in arbitrariness; they are: (1) personal whims precede the Sharīʿah objectives and (2) the use of permissible things in order to reach prohibited outcomes. If infringement is taken in its broadest sense, arbitrariness is regarded as a part thereof. The difference between taʿaddī and taʿassuf is that the former happens when a person intervenes without right or legal justification while the latter refers to a legal or rightful act but is corrupted with an invalid motive or harmful consequence.
Negligence means action without meeting the standard of due care, thus ending in risk imposition to self or others. It happens by falling short in taking appropriate care to avoid causing harm in a standard that the circumstances demand from a reasonable and prudent person. Negligence is determined, as al-Zuhaylī (d. 2015 in Syria) expounded, if a person utilizes any of his rights but without due care and necessary precaution and inflicts harm on others, he is thus negligent and is accountable for the consequences (1989, 4: 36). There is no disagreement regarding the imposition of liability due to negligence.
Infliction of Harm is on a Legitimate Benefit Owned by the Right Owner
Ḍarar is considered only when it affects a legitimate benefit owned by the right person. The term "legitimate" in this context means that Sharīʿah approves the ownership of a particular subject and its benefits. In addition, this subject and benefit must be owned legally and validly. Therefore, if somebody builds a home on another person’s land, the landlord can destroy it, and he is not liable because the former did not own this properly, for example (Mawāfī, 1997, p. 859).
Having said this, spoiling the wine or pork of a Muslim is not considered ḍarar. Another example is that a person is not held liable for the destruction of instruments that are used for illegal entertainment or tools which are used for only infliction of harm. However, if the wine or pork is owned by a non-Muslim, then their destruction will make a person accountable because they are properties of value (māl mutaqawwim) for a non-Muslim (Ibn ʿAbd al-Barr, 1992, 20: 161). According to the dominant opinion of the Shāfiʿī School, if a Muslim wrenched the wine of a Muslim, he is not obliged to give it back if he did not spoil it.
Although the destruction of prohibited things owned by a Muslim will not make a person liable, this procedure is not to be enacted by the public, but concerned authorities or legally appointed individuals have to carry out the task. Otherwise, it may lead to much havoc and disorder in society.
To sum up, harm means the violation of a legitimate interest, which fulfills the abovementioned four criteria. In fiqh, all types of harm need to be eliminated. Harm elimination is placed in three hierarchical layers. The first duty is the prevention of harm before its occurrence. The second is the elimination of the harm once it has occurred. The third is the minimization of the harm if the complete removal is impractical (Muhsin et al., 2019).
Medical Confidentiality from an Islamic Jurisprudence Perspective
Islamic jurisprudence (fiqh) gives high importance to privacy and dignity as basic human rights. The texts from the Quran and hadith demand respect for individual privacy by prohibiting any intrusion and access without consent. In addition, they substantiate that if anyone breaches privacy, he will be accountable here and in the hereafter.
As far as medical confidentiality is concerned, both earlier and contemporary Islamic jurists assert that its observance is an obligatory duty upon all healthcare professionals. In fiqh, the legal ruling on medical confidentiality is built on two premises, which are: (1) all secrets need to be concealed, and (2) the medical contract between doctor and patient requires the maintenance of confidentiality, and fulfilment of the contract is a mandatory duty. Fiqh regards respect for privacy as crucial for every individual to uphold his dignity and social standing. The Prophet stated that “a believer in (his or her) entirety is inviolable to another: his blood, his wealth and his honour” (Muslim, 2011).
In fiqh, a matter becomes medical confidential information if: “(1) a health worker gathers the information as a part of his profession, (2) the patient demands for concealment, and (3) the information is unknown to the public” (Muhsin, 2021, p. 3230). In fiqh, observance of medical confidentiality is not an absolute duty, but at times, as a final option, disclosure is allowed if necessary to avoid serious harm. The Islamic Fiqh Academy explained disclosure of patient privacy is allowed with restrictions in two scenarios. “Firstly, a breach is tolerated if the protection of confidentiality poses greater harm than the disclosure would. Secondly, a breach is accepted if it is in line with a public interest that outweighs the individual benefit gained from the protection of confidentiality” (The Islamic Fiqh Academy, 1993, Resolution No. 79/10/8). In Islam, some legal rules of prohibition, such as the prohibition of slander, are meant to protect people’s dignity and privacy (Muhsin, 2021, p. 3228). Respect for privacy has a direct implication for upholding dignity. Preservation of people’s dignity is deemed among the higher objectives of the Sharīʿah (maqāṣid al-Sharīʿah).
In their books related to medicine and medical ethics, Muslim scholars like Ishāq bin Ali al-Ruhāwī, al-Rāzī (d. 925 ad), Abdul Malik ibn Ḥabīb al-Andalūsī (d. 853 ad), Ibn Abī Uṣaybiʿah (d. 1270) and Aliyy ibn Riḍwān (d. 1061) unequivocally emphasized on the character of a doctor, his physical perfection, intelligence, competence, appearance, trust, and confidence. They asserted the importance of confidentiality in the doctor–patient relationship as it is a core factor for the delivery of effective healthcare. Some jurists like Ibn Qayyim (d. 1350) offered some vital discourses on the duties of physicians, including confidentiality (Ghalia et al., 2018, p. 145).
The Harm Elimination Principle in Medical Confidentiality
Most of the legal mandates and professional guidelines, if not all, acknowledge the protection of patients and others from serious harm as a valid justification to breach confidentiality. In addition, nearly all cases, wherein the breach of confidence is justified are based on the principle of eliminating the risk of serious harm to the patient or others in one way or another.
The Islamic ruling over the disclosure of privacy is based on the harm it produces. The prominent Muslim philosopher and jurist, al-Ghazālī (d. 1111), explained that the disclosure of privacy is a sign of disloyalty. Significantly, the disclosure is prohibited if it poses harm and it is a wicked act if it is disclosed without there being any risk of harm present. Amid the discussions regarding the rights of friends and colleagues, al-Ghazālī explained that they must conceal each other's secrets. A person can hide his weaknesses and secrets from others; likewise, he has to hide the secrets of his friends. Though they are physically two separate bodies, they share an emotional bond of friendship (Al-Ghazālī, 2005, 2: 1170). Public interest is generally regarded as a valid warrant for a breach of confidence. Whatever affects the life and liberty of citizens is considered a violation of public interest.
After explaining the "right to privacy" (see Article 8), the "Universal Declaration of Human Rights" draws some restrictions on this right (United Nations General Assembly, 1948). For example, disclosure is allowed if it is necessary to protect national interests and public safety. Likewise, privacy rights are sacrificed if a breach is essential in protecting the rights and liberties of citizens. Similarly, in the guidelines of the General Medical Council (GMC), UK, protection of a person from serious harm is considered a justified reason to breach patient confidentiality (2017). It further clarifies that if the disclosure puts the patient at stake, the doctor has to make an informed decision after weighing the possible harms of confidentiality with the potential benefits of disclosing patient information. In order to substantiate the "protection of the patient and others from harm" as a valid justification for the breach of confidentiality, the researcher presents Table 1, which outlines the exceptions for medical confidentiality observance in various medical codes of practice or ethical guidelines for medical practitioners.
Table 1 proves that the prevention of serious harm is a generally recognized exception for confidentiality breaches regardless of regional differences. In Table 1, the mentioned countries are from various parts of the world, including Islamic and non-Islamic countries. However, all of them consider the prevention of serious harm a valid justification to breach medical confidentiality.
The intrusion into a patient's privacy generally impacts two of his key interests. Firstly, it impinges on his interest to maintain the privacy of his relationship with the healthcare professional. It imperils the integrity of their therapeutic bond. This is because of a contingent condition, whereby if the patient believes that his private information will be shared with others against his wishes, he may withdraw from treatment, thus causing harm to his health as well as to others. Secondly, it encroaches upon his interest to avoid harms that may result from disclosure (Scott, 2001, p. 13).
Notably, the victims of the potential harm from the maintenance or disclosure of confidentiality in healthcare can be the patient, a physician, a third party, or the public. Harm to the patient can occur in numerous ways, including embarrassment, humiliation, social stigma, marital discord, loss of reputation, dismissal from employment, and denial of insurance. The list of harm extends further as it can also comprise legal jeopardies, loss of loved ones, mental depression, etc. (Beauchamp & Childress, 2001, p. 308). Similarly, the harm to third parties and the public consists of harm encompassing but not limited to, encroachment on physical integrity, violation of public interest and so on. As far as the harm to health workers is concerned, it includes breach of legal and statutory requirements, deterioration of the therapeutic relationship and loss of public confidence in the confidential approaches of the medical profession. In addition, the harm to healthcare professionals includes threats to his personal safety (World Health Organization, 2022). Causes of violence against healthcare professionals include depression, misunderstandings, grievances related to treatment, agitated mental disease, deep dissatisfaction, breach of confidentiality, malpractice, medical negligence, etc. At the heart of this problem is the deteriorating relationship between the doctor and the patient.
As explained in the previous section, the Sharīʿah gives due consideration to the probability and magnitude of harm when issuing the ruling of prohibition upon potentially harmful acts. The Islamic jurists consider an action or inaction as considerable harm when it is real or highly potential and excessive (fāḥish). From the Sharīʿah perspective, the severity of harm in medical confidentiality cases intensifies if it goes against the interests related to the ḍarūriyyāt of the maqāṣid, which are matters related to religion, life, health, family, intellect, wealth, and dignity. Based on the infliction of harm to the ḍarūriyyāt, harm is classified into physical, psychological, familial and financial aspects and those related to dignity. However, there are many healthcare cases in which maintaining medical confidentiality may cause various types of harm. For example, keeping the secret of an HIV-infected patient might concurrently result in physical, familial and financial harm.
In order to have a precise apprehension of potential harm in the discourse of medical confidentiality, harm is classified by theorizing inductively in light of rich pragmatic illustrations and reasoned facts into two: (1) harm that occurs due to maintenance of confidentiality and (2) harm that emerges as a consequence of disclosure. As part of dealing with the situation where the elimination of one harm entails the emergence of another, a professional has to be competent in understanding the differences among the types of harm and their gravity in light of Sharīʿah and established ethics, in order to be able to decide which harm to remove and which harm to compromise with. In the section below, after explaining consent and its importance in medical confidentiality disclosure, the author delves into serious infectious diseases and underlying types of harm in the practice of medical confidentiality.
Consent
The importance of consent in the discussion on potential harms in medical confidentiality is that it is a major medium to overcome many types of harm in the protection and disclosure of patient confidentiality. In order to minimize problems surrounding the disclosure of patient details, legal, and medical guidelines suggest seeking explicit consent for disclosure from the patient. However, although seeking consent helps to overcome ethical dilemmas on some occasions, at other times seeking consent puts people at the stake of harm or undermines the purpose of disclosure, such as in the case of preventing crime.
The explicit consent is granted when the patient clearly expresses, orally or through written format, that he has no objection to releasing the report to anyone or to particular individuals (Nujaydah, 1992, p. 203). Conversely, implicit consent is granted if the patient gives clear signs through an incident, circumstance, or situation, such as entering the consultation room with his/her partner, or appointing one’s son as a surrogate decision-maker. In other words, when it seems reasonable to infer the patient’s consent based on his actions, it is regarded as implicit (Qāyid, 1987, p. 458). In both cases, the usage of patient information is allowed only for the purposes for which consent is given.
In Islamic jurisprudence, for the consent to be valid in healthcare, the following conditions should be met: first, the consent has to be made with complete freedom and the patient must be in a state of full consciousness; second, the consent for disclosure should be from the patient himself; third, it should be given before the disclosure; and fourth, the consent has to be explicit or implicit with evidence (al-Najjār, 1990, p. 371).
Likewise, health workers have to give information promptly to an appropriate responsible person or authority or surrogate decision-maker if he believes that a patient, who lacks the capacity to give consent, is experiencing, or is at risk of neglecting, physical, sexual or emotional abuse, or any other kind of serious harm unless it is not of overall benefit to the patient to do so. On such occasions, professionals must restrict the disclosure to what is necessary and on a strict "need to know" basis, after taking precautions to prevent harm to the patient’s privacy or dignity (Herring, 2008, p. 178).
Harm Versus Harm in the Medical Confidentiality Practice
An ethical dilemma arises when an agent faces two or more ethical courses of action that are morally justifiable from various angles, where each of them appears mutually exclusive and either of them must be chosen, compromising other options. Sometimes, both choices would appear ethically unacceptable; however, the agent is hard-pressed to choose one course of action due to the necessity he faces in that situation (Ong et al., 2012, p. 11). As a result, a healthcare professional, who repeatedly plays the role of a decision-maker, comes across several "paradoxical" situations in his clinical practice where he has to determine an overriding "ought" after specifying and balancing various interests.
Along with ensuring strict non-maleficence to the patient, a health worker is legally and ethically bound to eliminate harmful situations that are likely to befall a third party because of their decisions or interventions. Disclosure is, on some occasions, a legal or ethical requirement, not left at the discretion of the health worker, and thus it may end in unintended consequences (Robin, 2014). As a result, a physician is bound to stay committed to the obligational standards of his profession, which call for the protection of a patient's privacy. On the other hand, he is also responsible for third parties who are at high risk of imminent harm from the patient if the confidentiality is upheld. In some cases, a third party is necessarily granted access to a patient’s private details in order to protect the welfare of the patient. This is because that situation may not allow the patient to make an informed decision, or his decision may happen to be inharmonious to his own benefit. Consequently, the maintenance of confidentiality becomes detrimental to the effective treatment itself.
At times, doctors face ethical dilemmas in making a decision regarding the confidentiality of their patients when a third party enquires about them for a valid purpose. Doctors may not be clearly aware of the procedures when their patients visit them with obvious proof of their involvement in criminal activities. Likewise, doctors in Muslim majority countries find conflicting interests when they have to make decisions on patients with a pregnancy of illegal or extramarital relationships, due to religious, ethical, and professional factors. In addition, the higher objectives of the Sharīʿah such as the protection of family, lineage, and dignity will come into conflict, with issues related to extramarital affairs and adultery adding ethical dilemmas to the choices of a doctor.
Several conflicting opinions in biomedical ethics originated from the dichotomy of views regarding the arguments on paternalism and the autonomy of the patient. As far as the paternalistic view is concerned, which is grounded on the ethics of rights, the doctor is supreme in a therapeutic relationship in the capacity of being a knowledgeable person about the patient’s condition. The argument for the autonomy of a patient, inherited from the Enlightenment, gives superiority to autonomous decisions over any other power and assures respect for one’s self-fulfilment. Put it in another way, a patient is regarded as a partner or a client in a therapeutic relationship. However, autonomy is not absolute, but adjustable according to various legal interests and not even exclusive from paternalism; rather medical jurists have to balance them delicately in applied contexts. This conflict evidently will reflect in the distinction between paternalistic practice with the claim that confidentiality may be breached to benefit the patient and the autonomy of the patient (Laurie et al., 2019).
A challenging matter that aggravates the existing issue is that the disclosure to evade any harm may cause other types of harm, whereby a practitioner struggles to decide whether to maintain or disclose what is confidential. For example, fear of disclosure may deter people from seeking medical care, which has severe consequences on both their own health and the public. Likewise, a recent study revealed that due to the possibility of disclosure of a medical report, some patients unfairly request that the doctor write inaccurate medical reports, or not mention certain information in their report, as they are worried about the harms that may emerge out of their possible disclosure. The illegal "defensive measures" undertaken by patients themselves often raise an immense threat to the integrity of the doctor–patient relationship, as well as the validity of medical research based on health reports (Scott, 2001, p. 14).
Among ethicists, one group asserts that although confidentiality is a vital principle in the doctor–patient relationship, it has certain inherent limits and could be breached if there is a necessity to do so. Meanwhile, the other group takes a strong stance in favour of absolute adherence to confidentiality and that no breaches are allowed at any cost. The two main justifications for the stance on absolute confidentiality are that (1) it is instrumental for an effective therapeutic relationship and (2) doctors do not hold the duty of beneficence to third parties, so a breach of confidentiality is not justified at the expense of harm to the patient (Ghalia et al., 2018, p. 153). However, on some occasions, absolute respect for confidentiality may result in generating greater harm than breaching confidentiality (Crook, 2013, p. 108). As a result, a healthcare professional faces a situation in which medical confidentiality requires trade-offs between the patient’s interest and the interest of others.
Below are some principles that at times conflict with each other when dealing with cases of confidentiality, i.e., when healthcare professionals are bound to adhere to two principles from various angles; however, they are mutually exclusive in the given scenarios (Table 2).
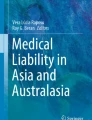
With regards to the target group, the conflict of interest could be portrayed as shown in Fig. 1.

Conflict of interest from the perspective of various obligations
As shown in the diagram, physicians face ethical dilemmas due to contradicting obligations to patients, legal mandates, professional guidelines, ethical codes, or third parties. For example, fulfilment of a doctor’s duty to patient confidentiality may end in his failure to do his duty to the third party by protecting him from a serious injury.
Harm Versus Harm in Confidentiality in Serious Infectious Diseases
Below is a brief discussion of "harm versus harm" in the practice of medical confidentiality of infectious diseases. Communicable diseases are a serious challenge in today’s world. It no longer needs explanation as the world is still struggling with the devastating repercussions of COVID-19. Notably, infectious diseases pose varying degrees of threat to the larger population. For instance, sexually transmitted diseases may pose a threat to particular individuals, whereas cases such as COVID-19 imperil a wider section of society within a shorter span of time. All forms of threats from infectious diseases require the appropriate (form of) disclosure in relation to the risk (Beauchamp & Childress, 2001, p. 298). All infectious diseases are not the same in terms of the perils involved in them, as some are fatal while others pose minimal type of harm.
As an example of a fatal communicable disease, issues in the confidentiality of HIV can be discussed. Infection of HIV is significant harm from an Islamic jurisprudence perspective as it fulfils all the criteria discussed in the above section. Therefore, its elimination is a mandatory religious duty upon Muslims. Over the past few decades, the disclosure of HIV to a sexual partner has been a frequent topic of considerable interest in debates relating to ethical and legal issues. The issue surrounding HIV notification is further aggravated, given that it triggers a conflict between mutually exclusive rights, which are (a) the patient’s right to confidentiality and (b) the right of a third party to the protection of life, which comes into effect when an HIV-infected patient refuses to reveal his condition to his sexual partner or to others who are at high risk of transmission (Herring, 2008, p. 225). In light of empirical studies, a sexual partner of an HIV-infected patient is at risk of having AIDS transmitted via unprotected sexual intercourse if the patient’s status is kept secret from the partner. Therefore, doctors strictly warn that HIV-infected patients refrain from unprotected sexual intercourse or other practices that are likely to result in the transmission of AIDS. In certain countries, if an individual deliberately (or recklessly without intention) infects another individual with HIV, he can be charged with a criminal offence and civil liability, as the offence satisfies the elements of fraud and severe bodily harm (Säfken & Frewer, 2007, p. 313). Some scholars argue that the breach of confidentiality is not permissible as long as the sexual activity is between consenting adults (Chenneville, 2000, p. 661).
As a general rule of thumb, it is suggested that the standard principles used in confidentiality should be applied to HIV cases, allowing for the disclosure of information pertaining to HIV-positive results to third parties if they are at risk of harm. In the case of contagious diseases, patients, at times, lose not only their right to privacy but also their right to autonomy over their daily life. This is because sometimes they will be forced into confinement, treatment and/or immunization (Emson, 1988, p. 88).
Doctors are responsible for reporting epidemiological information on communicable diseases. In clinical practice, notification of a communicable disease is justification for breaching confidentiality, which is arguably meant to protect public interests. In many national legal codes, the detection of communicable diseases obligatorily demands professionals to make a legally mandated breach of confidentiality, considering the risk to the remainder of society. However, from an ethical point of view, the professionals must take (in advance) some measures if the disclosure is likely to lead to a serious disadvantage to the patient in society. The concerns around public interest include enhancement of healthcare, public health surveillance, protection of innocent third parties, model law enforcement and the overall safety of a nation.
Likewise, if certain diseases are not treated with due care, an outbreak of infectious diseases can occur, leading to the deaths of thousands and/or resulting in huge financial liabilities. Therefore, it is the doctor’s duty to prevent the spread of infectious diseases which (in one way) can be achieved through their obligation of notification. For the prevention of harm infliction on the workforce, local health officials urge individuals suffering from infectious diseases to stay at home, in an attempt to prevent the spread of the disease to their colleagues and clients in the workplace. Consequently, the safety of the general public outweighs an individual’s interest when they conflict with each other.
Regarding infectious diseases, the Prophet said, “There is no ʿadwā (transmission of infectious diseases) and no ṭīrah (superstitious belief in bird omens) but I like good omens”. They (ṣaḥābah) asked, “What is a good omen (fa’l)?” He replied, “A good word” (Muslim, 2011). However, on another occasion, the Prophet said, “Flee from a leper as you would flee from a lion” (Al-Bukhārī, 2016). The scholars explain the reconciliation between the two ḥadiths, as the former denotes that no infection is caused without Allah’s command, and the latter guides people to take all possible precautionary measures to avoid infectious diseases. The Sunni Shafi'ite jurist and hadith scholar, al-Nawawī (d. 1277) explains that people with severe contagious diseases, like leprosy, are prohibited from socializing, entering the mosque, and using public water. He added that the people in that area should arrange and help infectious people to meet their needs such as facilities to get their water without socialization. He further explained that if no such facilities are arranged for the patients, they will not be barred from using the public spaces (2000, 14: 237).
In addition, some other Prophetic traditions also shed light on the duty of staying away from people who bear the risk of contagions (Muslim, 2011). In light of the above textual evidence, the Islamic jurists explain that considering the greater harm caused due to maintaining the confidentiality of an HIV-infected patient and other serious infectious diseases, doctors are obliged to disclose the relevant information to those at risk of infection (Nujaydah, 1992, p. 220).
Islamic scholars explain that the authority should enforce a ban on individuals with serious communicative diseases, which pose threat to other people’s health and life, from mixing with the wider public as well as to request them to relocate to separate living areas, as it is according to the Prophetic tradition. The notification of infectious diseases is an obligatory duty of healthcare professionals. Countries such as Saudi Arabia, Egypt, Jordan, and Iraq have made it obligatory for a healthcare professional to disclose information relating to infectious diseases.
In addition, prevention of all forms of harm to the human body is considered among the higher objectives of the Sharīʿah. As disclosure is often a vital medium in preventing major harms, the Sharīʿah recognizes its importance in the healthcare field and allows for it on certain occasions under specific rules and regulations. In the case of contagious diseases, the doctor is the supreme authority in determining its exactness as well as knowing the relevant individuals and officials who need to be informed in order to take the appropriate actions. Non-disclosure of an epidemic can result in jeopardizing more lives, which is clearly against the teachings and objectives of the Sharīʿah, as it is clear from the following verses: “Do not kill yourselves by adopting unlawful means” (al-Nisā’: 29) and “Let not your own hands throw you into destruction” (al-Baqarah: 195).
The following example illustrates potential harms that are likely to occur as a result of maintaining the confidentiality of an HIV-infected patient. A bisexual man, diagnosed as HIV-positive insists on his right to absolute confidentiality. He insisted his doctor not reveal his disease to anyone, including his partner; despite the efforts made by the doctor to caution the patient of the serious harm it will put his wife in, and the risk it will cause to their children in case of losing both of their parents to the disease. However, only a few weeks before his death, the patient allowed the doctor to disclose the disease to his wife; but by then, it was too late to save the wife from infection, as she has undergone a test, only to be diagnosed as HIV-positive. As a result, the wife accused the doctor of being negligent of the moral and legal obligations to her and her children (Gillet, 1987, pp. 15–20).
Concerning scenarios similar to the one mentioned above, some scholars argue that the doctor should try to convince the patient to disclose the information, and if he does not do so, the doctor should inform the partner of the infected person (Al-Ashqar, 2006, p. 103). In contrast, some other scholars view that the disclosure is not the duty of the doctor, but he should inform the patient of risks to others and advise him to disclose the information and to abstain from harming others. Here, the first opinion is preferred, since certain diseases are incurable, causing severe pain as well as irreparable harm to others, which can be mostly, if not entirely, prevented through disclosure. Regarding the issue of notification of infectious diseases, the majority of contemporary Muslim jurists opine that it is obligatory, though a few view it as not obligatory because notification is not a part of the medical profession (Tawfīq, 2006, p. 170). Prevention and elimination of significant harm is an obligatory duty upon all capable Muslims, from a fiqh perspective. In the situation of inflicting harm through serious infectious diseases, the healthcare professional is among the most capable to prevent and eliminate them.
The disclosure of an HIV infection, as discussed earlier, is primarily meant to prevent harm. However, if as a result of the disclosure, the infected patient refuses treatment and counselling, then this could lead to a state where the patient’s illness deteriorates and/or spreads to others through various means. Various kinds of individual troubles and social sufferings are also possible if the position of HIV-positive patients is made known to others (Robin, 2014, p. 54). According to some researchers who closely studied HIV patients, the disease itself causes far-reaching personal and social pains and its disclosure further escalates these pains. Some of the potential consequences are; social and sexual rejection by others, violence, gossip and invasion of privacy, harm to offspring, employment discrimination, exclusion, social ostracism, domestic tensions, fear, break-ups in relationships and a shameful sense of self and stigmatization (Robin, 2014, p. 54). Due to the knowledge that AIDS is a life-threatening illness, patients suffer severe psychological issues such as despair, anxiety, suicidal ideation, organic brain syndromes, anger, etc.
An incident occurred where a medical assistant revealed the medical report of a patient who had a sexually transmitted disease to colleagues of the patient, resulting in the patient undergoing an immense amount of distress and anxiety that required counselling and antidepressant medication. In this episode, apart from the mental depression and psychological dejection, the patient also incurred financial liabilities due to the medication required for her recovery from depression (NORCAL Group, 2017). Clearly, upon the breach of confidentiality and loss of dignity, a person first loses his peace of mind, which can lead to him suffering from severe mental depression.
Unlike HIV, some infectious diseases, like COVID-19, TB, and malaria, inflict harm to the public by spreading through open spaces. Tests are conducted as a major element in defensive medicine, which helps eliminate several types of harm and protects the general public. Firstly, it helps remove the epidemic before it spreads to the lives of many and also ensures that there is adequate treatment given to those who are affected by it, thus lessening the affliction of this contagious disease. Secondly, besides gathering baseline information about individuals at a particular place, tests and screening often offer direct benefits to the patient and the protection of others from infectious diseases. It is conducted with a higher purpose other than simply paternalistic purposes, which include saving a large number of people from fatal diseases. For example, if a patient with TB discontinues the proper treatment, this would cause the risk of the development of multi-drug resistant forms of the TB bacteria that could be a threat to the patient as well as others (Beauchamp & Childress, 2001, p. 300). As a consequence, along with health issues, individuals will suffer a financial burden. For public health practices and epidemiological investigations, health data are the lifeblood that can be useful in facilitating the rapid identification of necessities in healthcare and preventing outbreaks of deadly diseases. Privacy and public health are not at odds; rather, a balanced framework could be used, which is synergistic (Hodge, 2003, p. 663).
Upon disclosure, it is possible that the professions of certain individuals may be at risk. For example, a surgeon was diagnosed as HIV-positive at the medical centre where he practised. Within a few hours, he received several calls of sympathy from his colleagues and within days, his patients also conveyed to him their sympathy. Shortly after this, his surgical privileges were suspended and he lost his job. The above experience was of a doctor in the USA, who had expectations that his confidentiality would be upheld.
The above discussion clarifies that the disclosure, as well as the protection of confidentiality of serious infectious diseases, may pose significant harm to patients, doctors, and the public in one way or another. Tables 3, 4 and 5 show some of the potential harms of concealing and disclosing infectious diseases.
Tables 3, 4 and 5 substantiate that harm in the maintenance and disclosure of infectious diseases can be inflicted upon a patient, doctor, third party, society, and/or public’s interest. In addition, the potential harms are related to various categories, namely: moral, material, physical, psychological, financial, familial, professional, direct, indirect, private, and public.
As illustrated, the potential harms related to breaches of medical confidentiality are significant and serious from an Islamic jurisprudence perspective. As a result, its prevention, elimination, and minimization in unavoidable situations becomes an obligatory duty upon Muslims from a religious perspective. It is in addition to their professional and legal duty regarding the practice of medical confidentiality. It is also proved that in the light of Islamic legal maxims, a framework for harm elimination can be drawn that can be crucial in making decisions in the scenarios of ethical dilemmas and conflicts of interests (Muhsin et al., 2019). The author believes the implementation of the harm elimination framework has undeniable scope in resolving some of the complicated scenarios that may occur amid the practice of the medical confidentiality principle.
Conclusion
As a general standard of professional conduct, medical confidentiality is an inherent and imperative duty in medical practice. Healthcare professionals are obliged to protect the privacy of all information that they gather from their clients using the privilege of their profession. Notably, both in ancient and contemporary medico-ethical codes, the confidentiality principle is given due recognition, a fact that underscores the importance of the implementation of this principle.
In daily clinical routines, health workers are repeatedly confronted with the duty of confidentiality, as it conflicts with other ethical, legal, and professional obligations. Since confidentiality is a foundational tenet in medical practice and considering its near-absolute nature, disclosure can only be considered a final resort, when all other alternatives are exhausted.
The Sharīʿah’s concern for human emotions and feelings is obvious in its rulings. It underscores the importance of upholding the dignity and privacy of human beings and prohibits all illegitimate invasions of privacy. Based on the textual evidence and juristic explanations, confidentiality observance is an obligatory duty in the healthcare milieu and, inexcusable disclosure of and illegitimate access to patient private information are prohibited. The prohibition of a confidentiality breach is primarily meant to protect a person and his relatives from the actual or potential harm that may befall them.
Fiqh does not rule all types of disruption on benefit as an infliction of harm that needs to be eliminated. Rather, the jurists place some criteria which need to be met for significant harm. The major four criteria are (1) harm has to be real or highly possible in the future, (2) harm has to be excessive, (3) infliction takes place because of infringement or arbitrariness or negligence and (4) infliction of harm is on a legitimate benefit owned by the right owner.
The disclosure of medical confidentiality mainly violates two key interests of the patients: (1) integrity of therapeutic bond and (2) patients’ interest to avoid harms that may result from a disclosure. In Sharīʿah, medical confidentiality is not an absolute principle, rather it has limitations, thus it can be breached when the maintenance of confidentiality causes serious harm or contradicts an overriding principle.
Among specific matters which permit the disclosure of medical confidentiality is the protection of patients and others from serious harm, which is a recognized exception by several professional bodies in various countries. However, the doctors face situations where maintenance of confidentially conflicts with other similar or overriding principles. In addition, on some occasions, disclosure for the prevention of serious harm happens to be a reason for another harm whereby a practitioner struggles to decide whether to maintain or disclose what is confidential.
The exploration of relevant cases proves that there are situations where the maintenance and disclosure of medical confidentiality result in harm infliction. These types of harm are serious and significant from the view of Islamic jurisprudence because they meet the criteria of a considerable harm. Therefore they need to be addressed with due importance. In addition, it asserts that harm can be inflicted upon the patient, doctor, third party, society, and/or public’s interest. The potential harms are not of one type but they include various categories, namely moral, material, physical, psychological, financial, familial, direct, indirect, private, and public harms.
References
ʿAbd al-Ra’ūf al-Manāwī. (1937). Fayḍ al-Qadīr sharḥ al-Jāmiʿ al-Ṣaghīr. Cairo, Egypt: Maṭbaʿat Muṣṭafā Muḥammad.
Al-Ashqar, S. (2006). "Ifshā’ al-Sirr fī al-Sharīʿah al-Islāmiyyah." In Paper presented at Nadwat al-Ru’yah al-Islāmiyyah li baʿḍ al-Mumārasāt al-Ṭibbiyyah, Kuwait, 2006.
Al-Bukhārī, M. b. I. (2016). al-Jāmiʿ al-Ṣaḥīḥ. al-Bushra.
Al-Ghazālī, A. Ḥ. (1993). al-Mustaṣfā min ‘Ilm al-Usūl. Beirut, Lebanon: Dār al-Kutub al-’Ilmiyyah.
Al-Ghazālī, A. Ḥ. (2005). Iḥyā’ Ulūm al-Dīn. Beirut, Lebanon: Dar Ibn Hazm.
Al-Ḥaṣkafī, M. b. ʿA. (2002). Al-Durr al-Mukhtār Sharḥ Tanwīr al-Abṣār. Beirut, Lebanon: Dār al-Kutub al-ʿIlmiyyah.
Al-Kāsānī, ʿA’ al-D. (1986). Badā’iʿ al-Ṣanā’iʿ fī Tartīb al-Sharā’iʿ. Beirut, Lebanon: Dār al-Kutub al-ʿIlmiyyah.
Al-Khafīf, ʿA. (2000). Al-Ḍamān fī al-Fiqh al-Islāmī. Beirut: Lebanon: Dār al-Fikr al-ʿArabī.
Al-Kufawī, A. b. M. (2010). Al-Kulliyāt Muʿjam fī al-Muṣṭalaḥāt wa al-Furūq al-Lughawiyyah. Mu’assasat al-Risālah.
Al-Najjār, ʿA. A. M. (1990). al-Ḍarar al-Adabī wa Madā Ḍamānuhu fī al-Fiqh al-Islāmī wa la-Qānūn: Dirāsah Muqararanah. Dār al-Nahḍah al-ʿArabiyyah.
Al-Nawawī, M. al-D. (2000). Sharaḥ al-Nawawī ʿalā Ṣaḥīḥ Muslim (7th ed.). Beirut, Lebanon: Dār al-Maʿrifah.
Al-Rāzī, F. al-D. (1979). al-Maḥṣūl. Jāmiʿat al-Imām Muḥammad bin Saʿūd.
Al-Shāṭibī, A. I. (2004). al-Muwāfaqāt. Beirut, Lebanon: Dār al-Fikr al-ʿArabī.
Al-Tusūlī, ʿA. b. ʿA. al-S. (1998). al-Bahjah fī Sharḥ al-Tuḥfah. Beirut, Lebanon: Dār al-Kutub al-ʿIlmiyyah.
Al-Zuhaylī, W. (1989). al-Fiqh al-Islāmī wa Adillatuhu. Amman, Jordan: Dār al-Fikr.
American Medical Association. (2018). Opinions on privacy, confidentiality and medical records. AMA Code of Medical Ethics Opinions on Privacy, Confidentiality and Medical Records. AMA. Retrieved November 22, 2022, from https://www.ama-assn.org/sites/default/files/media-browser/code-of-medical-ethics-chapter-3.pdf.
Beauchamp, T., & Childress, J. (2001). Principles of biomedical ethics (5th ed./6th ed.). Oxford, UK: Oxford University Press.
Chenneville, T. (2000). HIV, confidentiality, and duty to protect: A decision-making model. Professional Psychology: Research and Practice, 31(6), 661–670. https://doi.org/10.1037/0735-7028.31.6.661
Crook, M. A. (2013). The risks of absolute medical confidentiality. Science and Engineering Ethics, 19(1), 107–122. https://doi.org/10.1007/s11948-011-9283-1
Dubai Health Authority. (2019). Code of ethics and professional conduct of Dubai Health Authority. Health Regulation Sector. Dubai Health Authority. Retrieved November 22, 2022, from https://www.dha.gov.ae/uploads/112021/a418db0a-991e-475f-99b1-c0062df0b228.pdf
Emson, H. E. (1988). Confidentiality: A modified value. Journal of Medical Ethics, 14(2), 87–90. https://doi.org/10.1136/jme.14.2.87
General Medical Council. (2017). Disclosing patients’ personal information: A framework. Retrieved November 22, 2022, from https://www.gmc-uk.org/ethical-guidance/ethical-guidance-for-doctors/confidentiality/disclosing-patients-personal-information-a-framework
Ghalia, B., Amanullah, M., Zakariyah, L., & Muhsin, S. M. (2018). Medical ethics in the light of Maqāṣid Al-Sharīʿah: A case study of medical confidentiality. Intellectual Discourse, 26(1), 133–160. Retrieved November 22, 2022, from https://journals.iium.edu.my/intdiscourse/index.php/id/article/view/1118
Gillet, G. (1987). AIDS and confidentiality. Journal of Applied Philosophy, 4(1), 15–20. https://doi.org/10.1111/j.1468-5930.1987.tb00198.x
Herring, J. (2008). Medical law and ethics (2nd ed.). Oxford, UK: Oxford University Press.
Hodge, J. G. (2003). Health information privacy and public health. Journal of Law, Medicine and Ethics 31(4), 663-671. https://doi.org/10.1111/j.1748-720X.2003.tb00133.x
Ibn ʿabd al-Barr, A. ʿU. Y. (1992). Al-Kāfī fī Fiqh al-Madīnat al-Mālikī. Beirut, Lebanon: Dār al-Kutub al-ʿIlmiyyah.
Ibn Fāris, A. al-Ḥ. A. (1991). Muʿjam Maqāyīs al-Lughah. Ed: ʿAbd al-Salām Muḥammad Hārūn. Dār al-Jīl.
Indian Medical Council. (2002). Professional Conduct, Etiquette and Ethics Regulations 2002. Indian Medical Council. Retrieved November 22, 2022, from https://wbconsumers.gov.in/writereaddata/ACT%20&%20RULES/Relevant%20Act%20&%20Rules/Code%20of%20Medical%20Ethics%20Regulations.pdf
Kamali, H. (2003). Principles of Islamic jurisprudence. Cambridge, UK: The Islamic Texts Society.
Laurie, G., Harmon, S., & Dove, E. (2019). Mason and McCall Smith's law and medical ethics (11th ed.). Oxford, UK: Oxford University Press.
Mawāfī, A. (1997). Al-Ḍarar fī al-Fiqh al-Islāmī: Taʿrīfuhu, Anwāʿuhu ʿAlāqātuhu, Ḍawābituhu, Jazā’uhu. Dār Ibn ʿAffān li al-Nahsr wa al-Tawzīʿ.
Medical and Dental Council of Nigeria. (2018). Code of medical ethics in Nigeria. Retrieved November 22, 2022, from https://www.mdcnigeria.org/downloads/code-of-conducts.pdf
Muhsin, S. M. (2021). Medical confidentiality ethics: The genesis of an Islamic juristic perspective. Journal of Religion and Health 61(4), 3219–3232. https://doi.org/10.1007/s10943-021-01313-7
Muhsin, S. M., Amanullah, M., & Zakariyah, L. (2019). Framework for harm elimination in light of the Islamic legal maxims. Islamic Quarterly, 63(2), 233–272. ISSN 0021-1842.
Muslim, A. al-Ḥ. (2011). Ṣaḥīḥ Muslim. Dār al-Jīl wa Dār al-Ᾱfāq al-Jadīdah.
NORCAL Group. (2017). Patient confidentiality: Understanding the medical ethics issues. Retrieved November 22, 2022, from https://www.norcal-group.com/library/patient-confidentiality-understanding-the-medical-ethics-issues
Nujaydah, ʿA Ḥ. (1992). Iltizāmāt al-Ṭabīb fī al-ʿAmla al-Ṭibbī. Dār al-Nahḍah al-ʿArabiyyah.
Ong, W. U., Yee, C. M., & Lee, A. (2012). Ethical dilemmas in the care of cancer patients near the end of life. Singapore Medical Journal, 53(1), 11–16.
Pakistan Medical and Dental Council. (2011). Code of Ethics of Practice for Medical and Dental Practitioners. Retrieved November 22, 2022, from https://pakistanlawyer.com/2016/06/14/code-of-ethics-of-practice-for-medical-and-dental-practitioners-regulations-2011/
Powers, P. R. (2006). Intent in Islamic law, motive and meaning in medieval Sunnī fiqh. Leiden, Netherlands: Brill.
Qāyid, U. (1987). Al-Mas’ūliyyat al-Jinā’iyyah al al-Ṭabīb ʿan Ifhsā’ al-Sirr al-Mihnah: Dirāsah Muqāranah. Cairo, Egypt: Dār-Nahḍah al-ʿArabiyyah.
Säfken, C., & Frewer, A. (2007). The duty to warn and clinical ethics: Legal and ethical aspects of confidentiality and HIV/AIDS. HEC Forum, 19(4), 313–326. https://doi.org/10.1007/s10730-007-9051-4
Scott, C. (2001). Is too much privacy bad for your health. In J. M. Humber & R. F. Almeder (Eds.), Privacy and health care. Totowa, NJ: Humana Press.
Shubayr, M. ʿU. (2007). Al-Qawāʿid al-Kulliyah wa al-Ḍawābiṭ al-Fiqhiyyah fī al-Sharīʿat al-Islāmiyyah (2nd ed.). Dār al-Nafā’is.
Siegler, M. (1995). Confidentiality in medicine: A decrepit concept. In C. Levine (Ed.), Taking sides in clashing views on controversial bioethical issues (6th ed.). Guiford, CT: The Dushkin Publishing Group, Inc.
Singapore Medical Council. (2016). Medical confidentiality. Ethical code and ethical guidelines. Retrieved November 22, 2022, from https://www.healthprofessionals.gov.sg/docs/librariesprovider2/default-document-library/2016-smc-ethical-code-and-ethical-guidelines---(13sep16).pdf
Tawfīq, Al-W. (2006). "Ḥukm ifshā’ al-Sirr fī al-Islām." Nadwat al-Ru’yah al-Islāmiyyah li baʿḍ al-Mumārasāt al-Ṭibbiyyah, Kuwait.
The Islamic Fiqh Academy. (1993). Resolutions and recommendations. In Eight Session in Bandar Seri Begawan, Brunei Darussalam, 1–7 Muharram 1414 AH (21–27 June 1993). Resolution No. 79/10/8.
The Malaysian Medical Council. (2011). Confidentiality. The Malaysian Medical Council. Retrieved November 22, 2022, from https://mmc.gov.my/wp-content/uploads/2019/11/Confidentiality-guidelines.pdf
The Nursing and Midwifery Council. (2002). Code of professional conduct. Retrieved December 31, 2022, from https://www.nmc.org.uk/standards/code/
The Saudi Commission for Health Specialties. (2014). Code of ethics for healthcare practitioners studies. The Saudi Commission for Health Specialties. Retrieved November 22, 2022, from https://www.iau.edu.sa/sites/default/files/resources/5039864724.pdf
United Nations General Assembly. (1948). Universal declaration of human rights. Paris. UN General Assembly. Retrieved November 22, 2022, from http://www.un.org/en/universal-declaration-human-rights/
Williams, J. R. (2015). Medical ethics manual (3rd ed.). Ferney-Voltaire Cedex, France: World Medical Association.
World Health Organization. (2022). Preventing violence against health workers. Retrieved November 22, 2022, from https://www.who.int/activities/preventing-violence-against-health-workers.
Acknowledgements
I thank the anonymous reviewers for their creative and critical comments on the earlier draft of this manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
I confirm that I have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Muhsin, S.M. Islamic Jurisprudence on Harm Versus Harm Scenarios in Medical Confidentiality. HEC Forum 36, 291–316 (2024). https://doi.org/10.1007/s10730-022-09503-w
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10730-022-09503-w